Content
The content of medical knowledge in this section of the site of the Lactology Foundation is intended for the practical needs of doctors, pharmacists and students in these specialties. It is more than reasonable to consult other authoritative medical sources before using our medical knowledge.
- Pulmonology
- Cardiology
- Nephrology
- Emergency medicine
- Gastroenterology
- Hematology
- Oncology
- Rheumagology
- Allergology
- Neurology and Neurosurgery
- Endocrinology
- Pharmacotherapy and other medical knowledge
Late Complications of Ulcer Disease
It is important to note that
gastric ulcers, much more
more
commonly than duodenal ulcers, can
be caused by
carcinoma.
Histologic diagnosis is therefore
man-
datory and the healing must
be monitored endos-
copically.
Pyloric Stenosis
Pyloric stenosis is a
late complication of chronic recurring ulcers.
The character of ulcer pain is changed and loss
of appetite occurs. Feelings of fullness and
discomfort after meals, which are not present in
uncomplicated ulcers indicate stenosis. A
stenosis is very likely with vomiting that
relieves or cures late pain and with vomiting of
food from the previous day. If endoscopic
examination identifies empty stomach secretion
and food 12 hours after eating, this supports
the diagnosis. Food and liquid retention can
often be detected by sonography. The diagnosis
is confirmed radiologically by slow pyloric
passage, dilatation of the stomach, and marked
dilution of the contrast agent by stomach
secretion and food residues. The nature of the
pyloric stenosis (benign or malignant) can
generally be defined by endoscopy and histology.
Gastric Carcinoma
Epidemiology and Risk
Factors. 85% of malignant tumors in the stomach
are adenocarcinomas. They can grow as
space-filling processes or diffusely infiltrate
the stomach wall (linitis plastica). Non-Hodgkin
lymphoma and leiomyosarcoma are malignant
gastric tumors. Nitrates in food, which are
converted to carcinogenic nitrites by bacteria,
play an important role in the development of
gastric carcinoma. Hp infection also seems to
play a significant role. Patients with chronic
atrophic type A gastritis are at particular risk
for carcinoma. Gastric carcinomas are more
frequent in patients with blood group A.
Clinical Features. In contrast to ulcers, the
symptoms of gastric carcinoma are less typical.
They start slowly, are uncharacteristic, and are
not periodic. There is generally no history of
stomach complaints. Typical features are the
persistence or progression of the complaints and
the appearance of general symptoms, particularly
weakness (anemia) and weight loss.
Iron-deficiency anemia frequently precedes the
local symptoms by weeks or months. In contrast
to ulcer symptoms, carcinoma pain
is not
relieved by antacids and is not periodic. In
about one-quarter of cases there is no pain, but
rather unspecific complaints (feeling of
fullness, discomfort, belching, nausea). In
other cases the complaints are more diffuse, e.
g., loss of appetite and weight loss. Vomiting
is typical for tumors in the antrum or cardia.
Cardiac carcinoma extending to the esophagus
typically causes dysphagia.
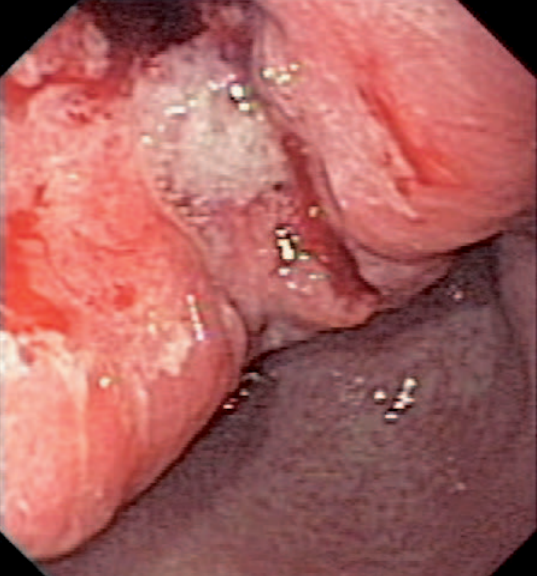
Exophytically growing ulcerated carcinoma in the prepyloric antrum (moderately differentiated adenocarcinoma).
Diagnosis. The carcinoma is generally
palpable only in advanced cases. The early cases
are either not sensitive to palpation or present
with diffuse pain. A Virchow gland above the
left clavicle is typical for advanced gastric
carcinoma.
Endoscopy and histology are
usually diagnostic. If endoscopy suggests
gastric carcinoma, a negative biopsy does not
rule out a carcinoma. Close
endoscopic-histologic monitoring is necessary
for early detection of gastric carcinoma.
Failure of an ulcer to heal after four to eight
weeks of medical therapy or early recurrence are
indications for a malignant or complicated
ulcer.
Detection of early cancer by endoscopy
improves prognosis. Early cancer, defined as
carcinoma restricted to mucosa and submucosa, is
generally cured by surgery.
Hematemesis
Causes. Hematemesis indicates
a bleeding mucosal lesion proximal to the
duodenojejunal flexure. The main causes of acute
upper gastrointestinal bleeding are:
➤ peptic
ulcers
➤ erosive gastritis
➤ Mallory−Weiss
syndrome
➤ esophageal varices.
In 80-90%
of all cases one of these four diseases is
present.
Mallory-Weiss syndrome is caused by
tears in the mucosa in the cardia region at the
gastroesophageal junction, which generally occur
during massive, cramp-like vomiting.
Other
uncommon causes of hematemesis are:
➤
esophagitis
➤ tumors of the gastroduodenal
region
➤ hemorrhagic diathesis
➤ hemobilia
➤ haemosuccus pancreaticus
➤ hemangioma
➤
Osler disease
➤ aortointestinal fistula
➤
mesenteric arterial occlusion
➤
pseudoxanthoma elasticum.
Hemobilia must be
suspected in hematemesis in association with
biliary colic or jaundice. The main cause is an
abdominal trauma with central or subcapsular
liver rupture. In some cases hemobilia may occur
months after the trauma. Liver abscess,
echinococcus infection, vascular anomalies,
liver tumors, and gallstone penetration are
other causes of hemobilia.
Melena
Causes. Massive tarry stools
generally have the same causes as hematemesis.
These are mainly:
➤ peptic ulcers
➤
erosive gastritis and Mallory−Weiss syndrome
➤ esophageal varices
➤ tumors.
Hematemesis
concurrent with melena indicates that the source
of the bleeding must be proximal to the jejunum.
Hematemesis may also be absent in bleeding from
the upper gastrointestinal tract. Among others,
NSAID therapy must be considered as the cause of
hemorrhage.
Stress ulcers (particularly after
surgical procedures, burns) and hemorrhage due
to anticoagulant therapy must be considered.
If melena and no hematemesis are present, all
rare sources of bleeding distal from the jejunum
must be included in the differential diagnosis.
Various factors affect the occurrence of melena:
volume of blood (> 50 mL), intestinal transition
time (< 8 h), and effect of hydrochloric acid
and intestinal flora on hemoglobin. Rectal
bleeding with bright red blood indicates
hemorrhage from the colon or distal small
intestine (e.g., tumors, diverticula, Crohn's
disease, ulcerative colitis, angiodysplasia). A
massive hemorrhage in the upper gastrointestinal
tract may also be associated with bright red
rectal bleeding in cases of accelerated
intestinal passage. Tarry stools are observed in
some cases with hemorrhage from the proximal
colon, particularly in cases of slow intestinal
passage. An hemorrhagic diathesis, mesenteric
arterial and venous thrombosis, or other
vascular diseases (e. g., aneurysms, cavernoma,
hemangioma) may cause intestinal bleed-
Eng.
The effects of specific drugs, particularly iron
formulation, charcoal preparations, or certain
foods in large quantities (e. g., red beets,
blueberries) may imitate melena.
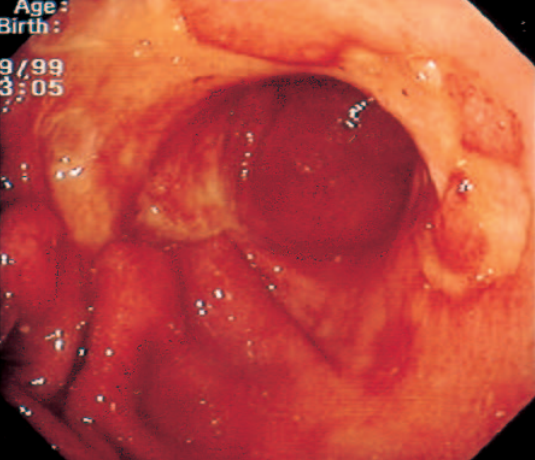
Non-Hodgkin lymphoma of the stomach.
Extensive
ulceration in the gastric antrum
and body; 70-year-old woman.
Diagnosis. Endoscopy is the method of choice
for detection and, if necessary, therapy. An
esophagogastroduodenoscopy followed by, if
necessary, a colonoscopy is generally indicated.
Angiography for the detection of abdominal
hemorrhage is restricted to cases with
continuous blood loss of 0.5−2.0 mL/min.
Small intestinal lesions, particularly tumors of
the small intestine, are difficult to detect. In
cases of intestinal bleeding with negative
endoscopic results, tumors of the small
intestine should be considered (e.g.,
schwannoma, leiomyoma, malignant lymphoma,
carcinoma). Capsule endoscopy and double balloon
enteroscopy are becoming increasingly important
in addition to radiologic small intestine
imaging, CT and MRI.
Uncommonly recurring
blood loss from the pancreas, particularly from
a pancreatic pseudocyst in chronic pancreatitis,
can be a diagnostic challenge (he-mosuccus
pancreaticus).
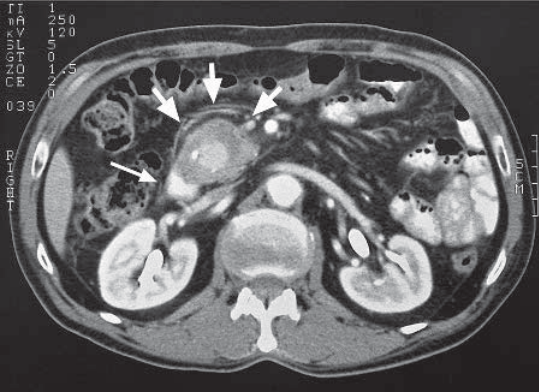
CT view of the pseudocyst in the head of the pancreas filled with contrast agent. The thin arrow points to a calcification, the thick arrows point to the pseudoaneurysm.
Rare Gastric Diseases
Malignant Lymphoma.
Malignant lymphoma is similar to gastric
carcinoma. Primary gastric lymphoma is rare.
However, the stomach is the most common
extranodal localization of a non-Hodgkin
lymphoma. The prognosis of malignant lymphoma is
significantly better than that of gastric
carcinoma. Infection with Hp is associated with
the development of gastric lymphoma,
particularly the MALT lymphoma. The eradication
of the Hp infection causes a regression of the
MALT lymphoma in about 50% of patients.
Lymphoma of the small intestine can also be a
complication of sprue
Leiomyoma. This tumor
is rare (approximately 1% of all tumors). The
most important clinical symptom is hemorrhage.
Endoscopy and radiography show a semispherical,
well-circumscribed tumor with central
ulceration.
Gastrointestinal Stromal Tumors
(GIST).
GIST are mesenchymal tumors of the
gastrointestinal tract, 60−
70% of which are
localized in the stomach. They were until
recently frequently classified as leiomyomas or
leiomyosarcomas, but have a specific cellular
origin and a specific pathogenesis. GIST are
identified by mutations of the cKIT
protooncogene and activation of the KIT receptor
tyrosine kinase, and like chronic lymphatic
leukemia, respond to treatment with the specific
ty-
rosin kinase inhibitor imatinib mesylate.
Intestinal Polyposis. In contrast to Ménétrier
disease, gas-
tric mucosa with intestinal
polyposis shows a predominantly normal, smooth
aspect with diffusely distributed individual
polyps at endoscopy. Gastric polyps are more
frequent in patients with chronic atrophic
gastritis, particularly in pernicious anemia.
The complaints are uncharacteristic. Depending
on the extent and location of the tumors, the
polyps may be asymptomatic, may present as
gastritis, or result in sudden stenosis. The
tumors often bleed, resulting in anemia that may
dominate the clinical picture. The diagnosis
must be histologically confirmed.
Hamartomatous polyps occur in the colon and the
small intestine in Peutz-Jeghers syndrome and
juvenile polyposis. Malignancy is rare compared
to familiar adenomatous polyposis, Gardner and
Turcot syndromes, and hereditary nonpolyposis
colorectal carcinoma.
Very Rare Gastric
Diseases. Syphilis, tuberculosis, sarcoidosis,
Crohn disease, eosinophilic gastritis, or
phlegmonous gastritis are extremely rare causes
of gastric complaints. Endoscopy and biopsy are
generally diagnostic. With many diseases the
diagnosis can only be confirmed if organs other
than the stomach are affected (e. g.,
sarcoidosis, Crohn's disease, tuberculosis).
Duodenal Diverticulitis. Duodenal diverticulitis
is generally harmless. Sometimes, however, it
may cause complaints similar to duodenal ulcers.
Annular pancreas must be considered in the
differential diagnosis. Periampullar or
intraduodenal diverticula originating from the
common bile duct may be a rare cause of
pancreatitis or cholangitis.
Please see also our Toxilact data base which is in the following language versions:
Toxilact Deutsche Sprachversion
Toxilact Nederlandstalige versie
Toxilakt έκδοση στην ελληνική γλώσσα
Toxilact English language version
Toxilact magyar nyelvű változat
Toxilact versione in lingua italiana
Toxilact polska wersja językowa
Detailed medical information on more common causes of acute abdomen
Intestinal Pain
Acute Appendicitis
Peritoneal Pain
Pain from Vascular Causes
Retroperitoneal Pain
Abdominal Pain from Intoxication
Toxicological risk during lactation
Toxicological lactation category I - the drug and/or its metabolites are either not eliminated through breast milk or are not toxic to the newborn and cannot lead to the development of absolutely any toxic reactions and adverse consequences for his health in the near and long term. Breast-feeding does not need to be discontinued while taking a given drug that falls into this toxicological lactation category.
Toxicological lactation category II - the drug and its metabolites are also eliminated through breast milk, but the plasma:milk ratio is very low and/or the excreted amounts cannot generate toxic reactions in the newborn due to various reasons, including degradation of the drug in the acid pool of the stomach of the newborn. Breastfeeding does not need to be discontinued while taking this medicine.
Toxicological lactation category III - the drug and/or its metabolites generate in breast milk equal to plasma concentrations or higher, and therefore the possible development of toxic reactions in the newborn can be expected. Breastfeeding should be discontinued for the period corresponding to the complete elimination of the drug or its metabolites from the mother's plasma.
Toxicological lactation category IV - the drug and/or its metabolites generate a plasma:milk ratio of 1:1 or higher and/or have a highly toxic profile for both the mother and the newborn, therefore their administration is incompatible with breastfeeding and it should to stop completely, and not just for the period of taking the drug, or to look for a less toxic therapeutic alternative.