Content
The content of medical knowledge in this section of the site of the Lactology Foundation is intended for the practical needs of doctors, pharmacists and students in these specialties. It is more than reasonable to consult other authoritative medical sources before using our medical knowledge.
- Pulmonology
- Cardiology
- Nephrology
- Emergency medicine
- Gastroenterology
- Hematology
- Oncology
- Rheumagology
- Allergology
- Neurology and Neurosurgery
- Endocrinology
- Pharmacotherapy and other medical knowledge
Intestinal Pain
Ileus
Ileus can be classified
into two main types:
➤ mechanical
ileus
➤ paralytic ileus
Mechanical Ileus
Clinical Features
Mechanical or obstruction ileus causes colicky
abdominal pain, frequently with periumbilical
localization. Intestinal colic, which results
from painful contraction of the intestine to
overcome an obstruction, lasts from seconds to a
few minutes. It can easily be distinguished from
urethral or gallstone colic, which lasts much
longer. Acute gas and stool retention always
indicates ileus and represents one of the most
important early symptoms together with pain and
possibly vomiting. Palpation of the abdomen
frequently triggers a colic.
Initially,
provided the intestinal wall is no longer
seriously damaged, there are almost no signs of
peritonitis, i. e., the abdominal pain is mild
and rebound tenderness is only minor. Signs of
inflammation are absent or mild (no or only mild
leukocytosis, normal ESR). The clinical picture
changes in later stages. The colicky pain
becomes continuous pain, and symptoms of
abdominal wall necrosis appear (peritonism,
leukocytosis, shock).
An asymmetric abdomen
indicates a localized intestinal distension
resulting from an organic obstruction (DD: acute
urinary retention).
Diagnosis
The bowel
sounds are initially increased on auscultation,
and disappear when, with time, the mechanical
ileus progresses to the paralytic stage.
Abnormal intestinal movements (stiffness), which
are caused by intestinal stenoses, can be
palpated in some cases or can be directly
observed during inspection of the abdomen. The
inconstant character is particularly typical.
Radiologically, the plain abdominal radiograph
shows distended intestinal loops with fluid
levels at an early stage. With colonic stenosis,
the proximal intestine is distended and the
haustra can be detected.
Distal to the
stenosis there is no air in the intestine.
Sonography can be helpful diagnostically by
demonstrating pathologic intestinal motility and
distended intestinal loops. The character of the
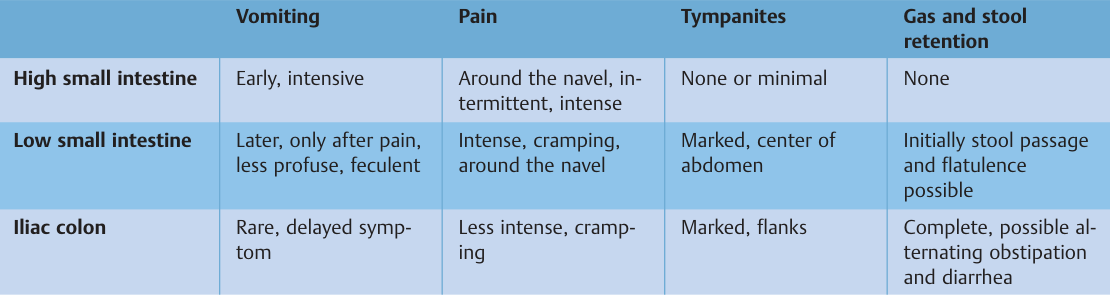
following four main symptoms enables
localization of the mechanical ileus.
➤
vomiting
➤ pain
➤ meteorism
➤ gas and
stool retention
Complications
If perfusion
of the intestinal wall is impaired due to
mechanical ileus, paralytic ileus with
continuous pain, localized peritonitis, shock,
and leukocytosis will occur. The blood pressure
is reduced, the pulse becomes rapid and weak.
Facies hippocratica with sunken cheeks develops.
Vomiting occurs in all stages. With complete
ileus fecal vomiting (copremesis) occurs. Gas
and stool retention are observed in most cases.
However, some patients also have diarrhea.
Causes of Mechanical Ileus
The most common
causes of mechanical ileus are previous
abdominal surgery (i.e., adhesions), neoplasms,
sliding hernia, volvulus, invagination, and
various other factors (e.g., foreign bodies,
Crohn disease, diverticulitis, mesenteric artery
infarction.
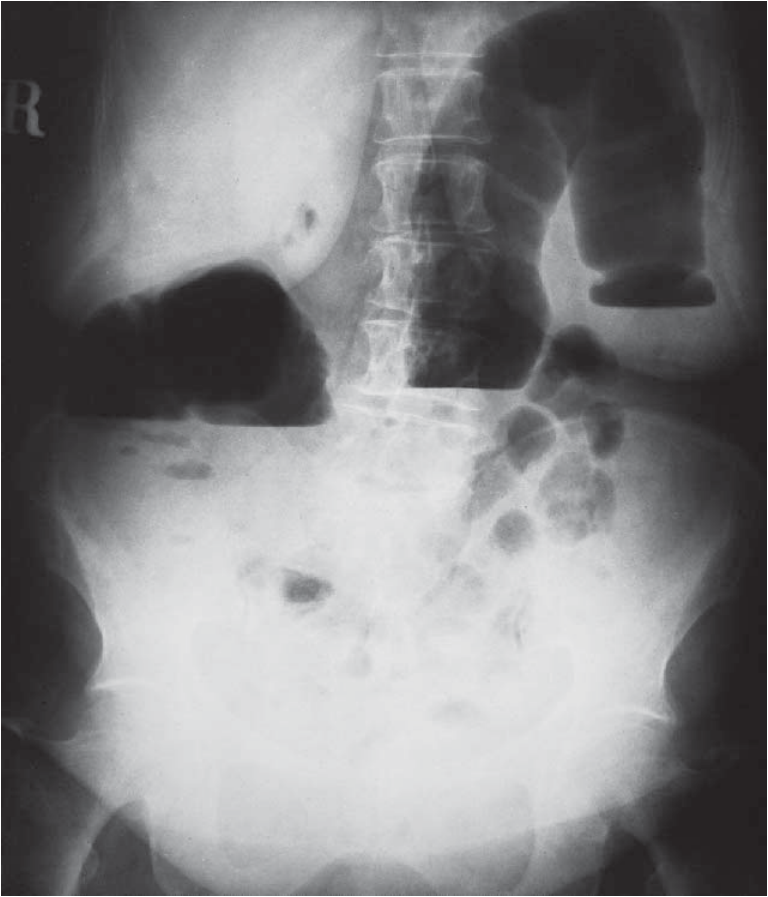
Mechanical ileus with seriously distended colon in a 73-year-old woman with carcinoma in the descending colon. Distal to the stenosis there is no air in the intestine.
Sliding hernias, postoperative adhesions (e.g., after appendectomy) or other surgical interventions, are frequent causes of a mechanical ileus. Therefore, sliding hernia and surgical scars must be considered in patients with an ileus. In children, and less frequently in young adults, an invagination and torsion of the intestine (volvulus) must also be considered. In both cases bloody stools are generally encountered. Obstruction of the intestine in adults is generally caused by a colorectal carcinoma. Carcinomas of the small intestine, which also cause ileus, are rare. In older patients with an acute abdomen a mesenteric infarction must be considered, which initially often presents with a clinical picture similar to that of mechanical ileus. Typical radiologic signs are gas-free intestines and later gas in the intestinal wall and portal vein.
Rarely, the horizontal
part of the duodenum is obstructed by the Treitz
ligament and the mesenteric arteries (superior
mesenteric artery; superior mesenteric artery
syndrome or mesenteric artery duodenal
compression). Postprandial vomiting of bile,
increased when standing or lying down, is the
most important indicator. Radiologic
demonstration of duodenal compression without
typical clinical symptoms is not sufficient to
diagnose duodenal obstruction. In adults the
diagnosis must be made only with great caution
and after exclusion of all other possible causes
(including irritable stomach).
Very rare
causes of a mechanical ileus are a large Meckel
diverticulum or endometriosis, which is
generally localized in the sigmoid colon. In
endometriosis the temporal association between
menstruation and occurrence of the symptoms will
result in the correct diagnosis. Passage of
gallstones into the intestine (biliary-digestive
fistula or more rarely via the common bile duct)
can cause an ileus (gallstone ileus). Lodging of
these gallstones most often occurs in the distal
or middle ileum, rarely in the jejunum, and
primarily affects older patients. Sonographic or
radiologic confirmation of air in the bile ducts
(pneumobilia) indicates a biliary-digestive
fistula and probably gallstone ileus. The
clinical−radiologic picture of the mechanical
small intestine (and colonic) ileus can also be
rarely caused by idiopathic intestinal
pseudoobstruction, which often occurs in waves.
Slow-onset abdominal colic with vomiting and
increasing meteorism and tendency to diarrhea
are typical symptoms. Radiologic diagnosis shows
distended intestinal loops and fluid in the
small and possibly the large intestine. However,
there are no signs of an intestinal stenosis
with no air distally. The episode frequently
subsides spontaneously within a few days.
Paralytic Ileus
Clinical Features
In paralytic ileus the
intestinal musculature is paralyzed while the
intestinal lumen is not obstructed. The
inhibition of the motor intestinal activity
prevents transport of the contents of the
intestine. Distension of the abdomen occurs and
it is painful upon pressure. Gases are not
emitted and intestinal sounds cannot be detected
by auscultation (deathly silence). In later
stages feculent, bilious and liquid stomach
contents may be vomited.

Mechanical small intestine ileus due to adhesions in a 70-year-old man (image taken in supine position).
Diagnosis
Distended
bowel loops with smooth wall contours and fluid
levels throughout the entire gastrointestinal
tract can be demonstrated by radiography.
Complications
Respiration is accelerated as a
result of intestinal intoxication and excessive
distension (diaphragm under high pressure).
Tachycardia, hypotension, and exsiccosis occur.
The face is sunken with halos around the eyes
and pale corners of the mouth being particularly
evident.
Causes of Paralytic Ileus
Common
causes of paralytic ileus are:
➤
postoperative (reflex intestinal atonia)
➤
peritonitis (e.g., after intestinal perforation)
➤ strangulation ileus
➤ serious infections
(Gram-negative sepsis)
➤ metabolic disorders
(uremia, diabetic coma)
➤ electrolyte
disorders
➤ pelvic or spinal fracture
➤
retroperitoneal diseases (e. g., pancreatitis,
hema-
Tom)
➤ mesenteric ischemia
➤
neurological disorders
Please see also our Toxilact data base which is in the following language versions:
Toxilact Deutsche Sprachversion
Toxilact Nederlandstalige versie
Toxilakt έκδοση στην ελληνική γλώσσα
Toxilact English language version
Toxilact magyar nyelvű változat
Toxilact versione in lingua italiana
Toxilact polska wersja językowa
Detailed medical information on more common causes of acute abdomen
Intestinal Pain
Acute Appendicitis
Peritoneal Pain
Pain from Vascular Causes
Retroperitoneal Pain
Abdominal Pain from Intoxication
Toxicological risk during lactation
Toxicological lactation category I - the drug and/or its metabolites are either not eliminated through breast milk or are not toxic to the newborn and cannot lead to the development of absolutely any toxic reactions and adverse consequences for his health in the near and long term. Breast-feeding does not need to be discontinued while taking a given drug that falls into this toxicological lactation category.
Toxicological lactation category II - the drug and its metabolites are also eliminated through breast milk, but the plasma:milk ratio is very low and/or the excreted amounts cannot generate toxic reactions in the newborn due to various reasons, including degradation of the drug in the acid pool of the stomach of the newborn. Breastfeeding does not need to be discontinued while taking this medicine.
Toxicological lactation category III - the drug and/or its metabolites generate in breast milk equal to plasma concentrations or higher, and therefore the possible development of toxic reactions in the newborn can be expected. Breastfeeding should be discontinued for the period corresponding to the complete elimination of the drug or its metabolites from the mother's plasma.
Toxicological lactation category IV - the drug and/or its metabolites generate a plasma:milk ratio of 1:1 or higher and/or have a highly toxic profile for both the mother and the newborn, therefore their administration is incompatible with breastfeeding and it should to stop completely, and not just for the period of taking the drug, or to look for a less toxic therapeutic alternative.