Content
The content of medical knowledge in this section of the site of the Lactology Foundation is intended for the practical needs of doctors, pharmacists and students in these specialties. It is more than reasonable to consult other authoritative medical sources before using our medical knowledge.
- Pulmonology
- Cardiology
- Nephrology
- Emergency medicine
- Gastroenterology
- Hematology
- Oncology
- Rheumagology
- Allergology
- Neurology and Neurosurgery
- Endocrinology
- Pharmacotherapy and other medical knowledge
Alopecia
Hair loss has a psychological
impact out of all proportion to its
physical significance, but disorders
causing hair fall may also sometimes
be a marker for systemic disorders.
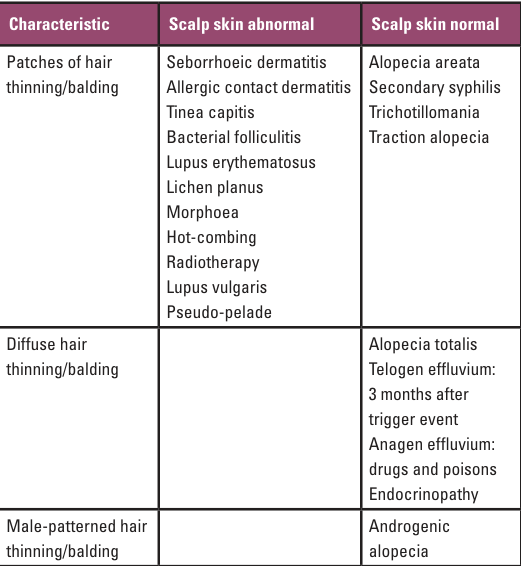
Convenient clinical division of the
possible causes of alopecia can be
made
by considering: (i) whether
or not obvious scalp skin
abnormality is present; and (ii) the
distribution of hair loss, for
example localized, generalized or
male-patterned.
PATCHY HAIR-THINNING/BALDING ACCOMPANIED BY
OBVIOUS SCALP SKIN DISEASE
Hair loss is
surprisingly uncommon in eczema and psoriasis of
the scalp, even when they are severe.
Allergic contact sensitivity to hair dye is a
common cause of a severe eczematous eruption of
the scalp, face and neck, but hair loss is
rarely a major feature. Small infants with a
severe generalized atopic eczema may produce a
patch of alopecia at the occiput through
habitual rubbing of the head on the pillow.
A child presenting with one or more localized
bald areas on the scalp associated with broken
stubbly hairs and scaling of the affected area
of the scalp is always suggestive of tinea
capitis (scalp ringworm) (see SCALP AND BEARD,
FUNGUS AFFECTIONS OF). The degree of surrounding
inflammation and scaling is very variable, and
depends on the fungus responsible, and the host
response. Cattle ringworm (Trichophyton
verrucosum) may produce a particularly violent
reaction, with swelling, discharge and local
lymphadenopathy, a condition termed a 'kerion';
direct microscopy of plucked hairs and
subsequent culture on Sabouraud's medium will
confirm the diagnosis.
Bacterial
folliculitis, if extensive enough, sometimes
perpetuated by infestation with head lice, can
cause patchy hair loss, sometimes with scarring
developing in late or neglected cases. Pustules
should be easily found, and there will be
draining lymphadenopathy. A sterile inflammatory
folliculitis (folliculitis decalvans) is a rare
cause of patchy balding in those who are
middle-aged.
Scarring alopecia
Various inflammatory
conditions of the scalp can result in
destruction of hair follicles by a scarring
process; in such cases, hair loss is inevitably
irreversible in the affected areas. Examination
of the surface of the scalp with a hand lens
reveals loss of follicles, and sometimes several
hairs emerging together from a single orifice.
Discoid lupus erythematosus and lichen planus
are common causes of scarring alopecia. More
esoteric causes include sarcoidosis,
radiotherapy, lupus vulgaris and pseudo-pelade.
If the scarring is linear, especially if it
extends to the forehead and has a violaceous
edge, localized scleroderma (morphoea) may be
the cause. The entire lesion has the appearance
of an exaggerated scar – en coup de sabre.

Lichen planus with scarring alopecia (Graham-Little syndrome).

Alopecia secondary to radiation.
PATCHY HAIR-THINNING/BALDING WITH NORMAL
UNDERLYING SCALP SKIN
Alopecia areata is the
most common cause of patchy baldness. Patches
are asymptomatic and are often discovered by
relatives or hairdressers. Patients of any age
are affected, especially those in late childhood
or early teens. The hallmark of this disease is
a neat, sharply localized patch of billiard-ball
baldness with no obvious inflammation or scaling
at the edge of lesions, and the diagnostic
exclamation mark hairs should be searched for.
There are usually two or three patches, and
sometimes these coalesce at an alarming rate and
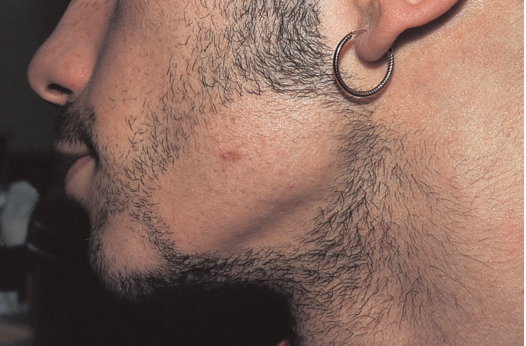
may even cause alopecia totalis of the scalp, or
alopecia universalis in which beard and all body
hair are lost. The course and prognosis are
highly variable but generally good. On average,
two or three patches appear, remain stable for
anything up to 6 months, and then regrow without
trace within 12 months. The regrowing hairs are
initially often white. The cause is unknown,
although there is a family history in 30 percent
of cases, and it is occasionally associated with
autoimmune diseases such as vitiligo, thyroid
disease, pernicious anemia or Addison's disease.
A convincing preceding history of emotional
shock is given by a proportion of patients, and
may be a triggering factor.
Alopecia areata - above
Syphilis, although relatively uncommon, is a
diagnosis that must not be overlooked. Patchy
alopecia may be a feature of the secondary
phase. The appearance is of an asymptomatic
patchy 'moth-eaten' baldness.
On examination,
there is no scaling or obvious scalp disease
and, in contrast to alopecia areata, baldness is
partial rather than complete. Exclamation mark
hairs are not seen, and the patches are more
numerous and accompanied by fever, sore throat
and
lymphadenopathy. The serology is
positive, and the hair regrows after antibiotic
treatment.
Trichotillomania is the rather
cumbersome title given to what often amounts to
only a 'habit tic'. If hair is twirled between
the fingers, it eventually breaks, leaving
patches of shortened hair. Microscopic
examination reveals obvious fractured ends of
the affected hair.
Some psychiatrically
disturbed individuals pursue hair pulling and
produce bald patches. The fractures may be seen
at the scalp surface, or even at the roots.
Traction alopecia is seen at the hair margins
and is due to regular hairdressing techniques,
for example rollers, braiding, ethnic plaiting
and tight pony tails, pulling on the hairs.

Traction alopecia - above.
DIFFUSE ALOPECIA WITHOUT SCALP DISEASE
Telogen effluvium
A growing (anagen) hair has
a large bulb, easily seen with a hand lens on
plucking. When growth stops, the bulb shrinks,
and the hair enters a resting (telogen) phase
for 3 months before falling (catagen). In
healthy adults, some 50–100 hairs enter telogen
daily, and thus fall some 3 months later. Not
surprisingly, certainly
events upset the hair
cycle, whereupon a larger number of hairs stop
growing and enter telogen.
Three months
later, they will fall as a so-called 'telogen
effluvium'.
Triggering events include
childbirth, stopping the contraceptive pill, a
febrile illness, blood loss, an operation,
myocardial infarction, stroke, rapid weight
loss, bereavement or other psychological stress.
The patient often complains of a worrying
increase in hair fall, but on examining the
scalp, no obvious abnormality is seen although,
if the hair is gently grasped between thumb and
finger, many telogen hairs may be detached.
Further evidence can be obtained
by asking
patients to collect their daily hair fall from
hair brushes and pillows. Normally, some 50–100
hairs can be collected, and 300–400 can fall
daily in telogen effluvium. The prognosis is
excellent.

Alopecia universalis - above.
Anagen effluvium
Fall of growing hairs
also causes diffuse hair-shedding, and may occur
after exposure to certain drugs or poisons, for
example cytotoxics, isotretinoin, thiouracil,
anticoagulants, excess vitamin A and thallium
poisoning.
Diffuse hair fall occurs in
endocrinopathy, for example myxoedema,
hypopituitarism and hypoparathyroidism.
Myxoedema is regularly accompanied by hair
thinning. The mechanism is unknown and may not
be directly related to serum thyroxine level, as
adequate replacement therapy may fail to reverse
the process. Hair loss may be a feature of
systemic lupus, and it may even be the
presenting symptom.
Male-pattern baldness without obvious scalp
disease
Male-pattern baldness is not a
disease, but an accelerated physiological
process, especially pronounced in those with a
genetic predisposition.
Males and females
progressively lose androgen dependent scalp
hairs with increasing age – in males with
successive thinning of the bitemporal, occipital
and pate areas, and in females with a more
diffuse patterned thinning over most of the
vertex. Some
individuals have increased
sensitivity of their hair follicles to normal
levels of circulating androgens, and lose their
androgen-dependent hair earlier. Such hair fall
does not occur in those who have been castrated,
and oestrogens and anti-androgenic drugs appear
to have a protective effect. The prognosis for
regrowth is
poor, although many individuals
search in vain for a cure.
Please see also our Toxilact data base which is in the following language versions:
Toxilact Deutsche Sprachversion
Toxilact Nederlandstalige versie
Toxilakt έκδοση στην ελληνική γλώσσα
Toxilact English language version
Toxilact magyar nyelvű változat
Toxilact versione in lingua italiana
Toxilact polska wersja językowa
Detailed medical information on more common causes of acute abdomen
Intestinal Pain
Acute Appendicitis
Peritoneal Pain
Pain from Vascular Causes
Retroperitoneal Pain
Abdominal Pain from Intoxication
Toxicological risk during lactation
Toxicological lactation category I - the drug and/or its metabolites are either not eliminated through breast milk or are not toxic to the newborn and cannot lead to the development of absolutely any toxic reactions and adverse consequences for his health in the near and long term. Breast-feeding does not need to be discontinued while taking a given drug that falls into this toxicological lactation category.
Toxicological lactation category II - the drug and its metabolites are also eliminated through breast milk, but the plasma:milk ratio is very low and/or the excreted amounts cannot generate toxic reactions in the newborn due to various reasons, including degradation of the drug in the acid pool of the stomach of the newborn. Breastfeeding does not need to be discontinued while taking this medicine.
Toxicological lactation category III - the drug and/or its metabolites generate in breast milk equal to plasma concentrations or higher, and therefore the possible development of toxic reactions in the newborn can be expected. Breastfeeding should be discontinued for the period corresponding to the complete elimination of the drug or its metabolites from the mother's plasma.
Toxicological lactation category IV - the drug and/or its metabolites generate a plasma:milk ratio of 1:1 or higher and/or have a highly toxic profile for both the mother and the newborn, therefore their administration is incompatible with breastfeeding and it should to stop completely, and not just for the period of taking the drug, or to look for a less toxic therapeutic alternative.