Content
The content of medical knowledge in this section of the site of the Lactology Foundation is intended for the practical needs of doctors, pharmacists and students in these specialties. It is more than reasonable to consult other authoritative medical sources before using our medical knowledge.
- Pulmonology
- Cardiology
- Nephrology
- Emergency medicine
- Gastroenterology
- Hematology
- Oncology
- Rheumagology
- Allergology
- Neurology and Neurosurgery
- Endocrinology
- Pharmacotherapy and other medical knowledge
ABDOMINAL SWELLINGS
These may be acute or chronic, general or local, and caused by abdominal accumulations that are gaseous, liquid or solid. They may arise in the abdominal cavity itself or in the abdominal wall.
SWELLINGS IN THE ABDOMINAL WALL
Swellings
located in the abdominal wall itself can be
recognized by their superficial position, by
their adherence to the skin, subcutaneous fascia
or muscles, or by their failure to follow the
movements of the viscera immediately underlying
the abdominal wall. It may be impossible to
differentiate, for obvious reasons, an
intra-abdominal mass that has become attached to
the abdominal parietes, either as an
inflammatory or malignant process. A simple test
that should be applied to all abdominal masses
is to ask patients to raise either their legs or
their shoulders from the couch. This procedure
tightens the abdominal muscles; if the lump is
intraperitoneal, it disappears, but if it is
situated in the abdominal wall itself it
persists.

A large subcutaneous lipoma in the epigastrium this moved freely on the anterior abdominal wall, even when the underlying muscles were tightly contracted, thus excluding the diagnosis of an epigastric hernia.
Inflammatory swelling of the abdominal wall
most commonly complicates a laparotomy incision,
and the diagnosis is obvious. A superficial
cellulitis may complicate infection of a small
abrasion or hair follicle infection.
Inflammation of the abdominal wall may be
secondary to an extension of an intraperitoneal
abscess, particularly an appendix abscess in the
right iliac fossa, or, on the left side, a
paracolic abscess in relation to diverticular
disease of the sigmoid colon or to perforation
of a carcinoma of the large bowel. Inflammatory
swelling of the umbilicus in newborn infants is
rare, except in primitive communities where the
cord is not divided with the niceties of modern
aseptic practice. Suppuration at the umbilicus
in adults is not uncommon if the navel is deep
and narrow.
A tender hematoma in the lower
abdomen may result from rupture of the rectus
abdominis muscle, or tearing of the inferior
epigastric artery, which may occur as a result
of a violent cough.
Tumors of the abdominal
wall are usually subcutaneous lipomas. These may
be multiple and may be a feature of Dercum's
disease (adiposa dolorosa).
Lipomas should be
carefully differentiated from irreducible
umbilical or epigastric hernias containing
omentum.
A desmoid tumor may arise in the
lower part of the abdominal wall, and malignant
fibrosarcomas or melanomas may also occasionally
be encountered.
A neoplastic deposit may
sometimes be palpated at the umbilicus and
represents a transcoelomic seeding, usually from
a carcinoma of the stomach or large bowel.
GENERAL ABDOMINAL SWELLINGS
Every medical
student knows the mnemonic of the five causes of
gross generalized swelling of the abdomen: Fat,
Fluid, Flatus, Faeces and Fetus.
In obesity,
the abdomen may swell either as a consequence of
the deposit of fat in the abdominal wall itself,
or as a result of adipose tissue in the
mesentery, the omentum and the extraperitoneal
layer. In very obese persons, it is rarely
possible to
diagnose the exact nature of an
intra-abdominal mass by the usual clinical
methods. Indeed, tumors of quite remarkable size
– including the full-term fetus – may remain
occult to even the most careful examiner.
Distension of the intestines with gas occurs in
intestinal obstruction and is particularly
marked in cases of volvulus of the sigmoid
colon, chronic large-bowel obstruction and
megacolon. It also occurs in adynamic ileus. The
whole of the abdomen, or in special cases some
part of it, is distended and gives on percussion
a highly resonant or tympanitic note. The
outlines of the gas-distended viscera are often
visible; loops of dilated small bowel, one above
the other, may produce a characteristic 'ladder
pattern'. The increased size of the inflated
intestine may produce displacement of the other
viscera; the dome of the diaphragm is pushed up
into the chest, shifting the apex beat of the
heart upwards. The liver is similarly displaced.
The distended stomach may occasionally be gross
enough all but to fill the abdomen in very
advanced cases of pyloric stenosis and in acute
gastric dilatation.
The causes producing an
accumulation of liquid in the peritoneal cavity
can be listed as:
• Congestive cardiac failure
• Cirrhosis
• Nephrotic syndrome
• Carcinomatosis
peritonei
• Tuberculous peritonitis
In
severe cases of chronic constipation, abdominal
distension may result from the accumulation of
faeces in the large intestine, particularly
where megacolon exists. The scybala may be felt,
usually soft and plastic in the region of the
ascending colon, and hard and nodular in the
descending and sigmoid colon. Rectal examination
often reveals an enormous accumulation of
faeces. In some cases of tuberculous
peritonitis, semi-solid inflammatory masses may
bring about a general swelling of the abdomen.
General swelling of the abdomen may occur in
malignant disease involving the peritoneum due
to the growth of numerous secondary nodules in
addition to a concomitant ascites. Pseudomyxoma
peritonei may follow rupture of a pseudomucinous
cystadenoma of the ovary or of a mucocoele of
the appendix. The entire abdominal cavity
becomes distended with gelatinous material.
LOCAL INTRA-ABDOMINAL SWELLINGS
These may
be due to some general cause, or to a mass
arising in a specific viscus.
Swellings due
to general causes
Causes that ordinarily
produce general swelling of the abdomen may
sometimes give rise to only a local swelling.
Thus, with encysted ascites left after an acute
diffuse peritonitis or accompanying tuberculous
peritonitis, an accumulation of fluid bounded by
adhesions between the adjacent viscera may be
found
in any part of the peritoneal cavity,
most often in the flanks or pelvis. A reliable
history may be a clue to the nature of such a
mass, although its cause may not be revealed
until a laparotomy has been performed.
Abdominal swellings may occur in tuberculous
peritonitis resulting from the rolled-up, matted
and infiltrated omentum, doughy masses of
adherent intestine, or enlarged tuberculous
mesenteric lymph nodes. The amount of ascites in
such cases varies considerably from a gross
degree to almost complete absence (the
obliterative form). Discovery of a tuberculous
focus elsewhere in the body is support for the
diagnosis.
Hydatid cysts may occur in any
part of the abdominal cavity. They are usually
single. The liver – particularly the right lobe
– is the most common situation, and more rarely
the spleen, omentum, mesentery or peritoneum.
The cyst grows slowly and is spherical
except
in so far as it is molded by the pressure of
adjacent structures. It contains a clear fluid
in which hooklets, scolices and secondary or
daughter cysts detached from the walls of the
parent cyst may be found.
Unless large enough to cause mechanical
pressure, the single hydatid cyst gives rise to
little pain, or indeed to any complaint of any
kind. It may produce a smooth, rounded, tense
bulging of the overlying abdominal wall. It is
dull on percussion, and it may yield a 'hydatid
thrill', as may any other cyst; this thrill is
the vibratory sensation experienced by the rest
of the hand when, with the whole hand laid flat
over the tumor, a central finger is percussed.
Occasionally, there may be pain and fever due to
inflammation within these cysts, and rupture
into the peritoneal cavity may cause a severe
anaphylactic reaction. Rupture of a hydatid cyst
of the liver into a bile duct may cause jaundice
due to biliary obstruction by daughter cysts.
Hydatid disease is rare except in countries
where the inhabitants live in close association
with dogs that are the hosts of Taenia
echinococcus (Australasia, South America,
Greece, Cyprus and, in the British Isles, North
Wales). About one-quarter of patients
demonstrate eosinophilia. A complement fixation
test gives a high
degree of accuracy. X-rays
of the abdomen may reveal calcification of the
cyst wall in long-standing cases.
Any part of the abdomen may swell from the
formation of an abscess. A subphrenic abscess
following a general peritonitis is occasionally
large enough to produce an upper abdominal
swelling.
The patient is usually seriously
ill with a swinging fever, rapid pulse,
leucocytosis and all the general manifestations
of toxaemia. However, in this antibiotic era, an
increasing number of examples are being seen of
a more insidious and chronic progression of the
disease, with the onset delayed weeks or even
many months after the initial peritoneal
infection. X-ray examination, together with
screening of the diaphragm, is extremely useful,
and at least 90 percent of patients with
subphrenic infection have some abnormality on
this investigation.
On the affected side, the
diaphragm is raised and its sharp definition is
lost. Its mobility on screening is diminished or
absent. There is frequently a pleural effusion,
collapse of the lung base or evidence of
pneumonitis. About 25 percent of patients have
gas
below the diaphragm, frequently
associated with a fluid level. This gas is
usually derived from a perforated abdominal
viscus, but it is occasionally formed by
gas-producing organisms. On the left side, gas
under the diaphragm may be confused with the
gastric bubble. An important differential
feature is that the gas shadow of the stomach
rarely reaches the lateral abdominal wall;
however, if there is doubt, a mouthful of barium
is given in order to demarcate the stomach.
Ultrasonography and computed tomography usually
clinch the diagnosis.
Pus may localize in either the right or left
paracolic gutter or iliac fossa. On the right
side, this usually follows a ruptured appendix,
or occasionally a perforated duodenal ulcer. On
the left, a perforation of an inflamed
diverticulum or carcinoma of the sigmoid colon
is the usual cause. A large pelvic abscess
frequently extends above the pubis or into one
or the other iliac fossa from the pelvis and can
be palpated abdominally as well as on pelvic or
rectal examination.
About 75 percent result
from gangrenous appendicitis, and the remainder
follow gynecological infections, pelvic surgery
or any general peritonitis.
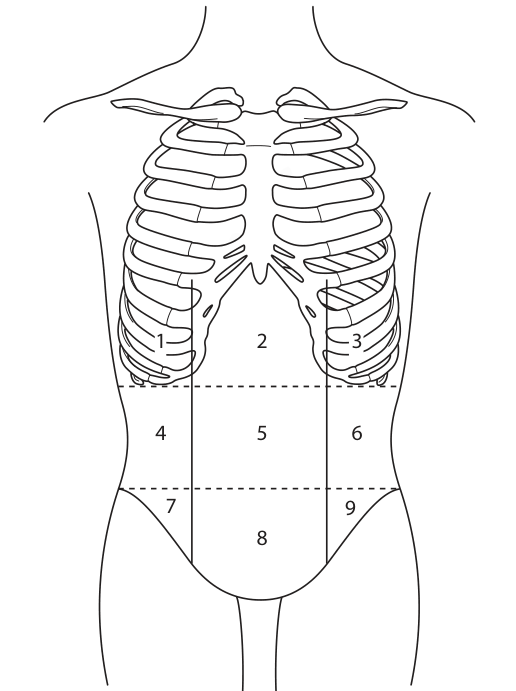
Regional diagnosis of local abdominal
swellings
For clinical purposes, the abdomen
may be subdivided into nine regions by two
vertical lines drawn upwards from the
mid-inguinal point midway between the anterior
superior iliac spine and the symphysis pubis,
and by two horizontal lines, the upper one
passing through the lowest points of the tenth
ribs (the subcostal line), the other drawn at
the highest points of the iliac crests – the
supra-cristal plane (Fig).
The three median
areas thus mapped out are named, from above
downwards, the epigastric, umbilical and
hypogastric (or suprapubic) regions; the six
lateral areas are, from above downwards, the
right and left hypochondriac, lumbar and iliac
regions. The abdominal swellings that may be
felt in and about these nine regions, excluding
the tumors located in the abdominal wall itself
that have already been described, are as
follows.
Right hypochondriac region
Most tumors in
this area are connected with the liver or
gallbladder.
An easily made mistake is to
regard the firm and rounded swelling produced by
the upper segment of the right rectus abdominis
muscle, especially in a well-developed subject,
as a tumor of the liver or gallbladder. In such
cases, the characteristic dull note of the liver
on percussion over the lower right chest ceases
at the costal margin.
Tumors in connection
with the hepatic flexure of the colon, scybalous
collections in the hepatic flexure region, or
the head of an intussusception may present as
masses in this area.
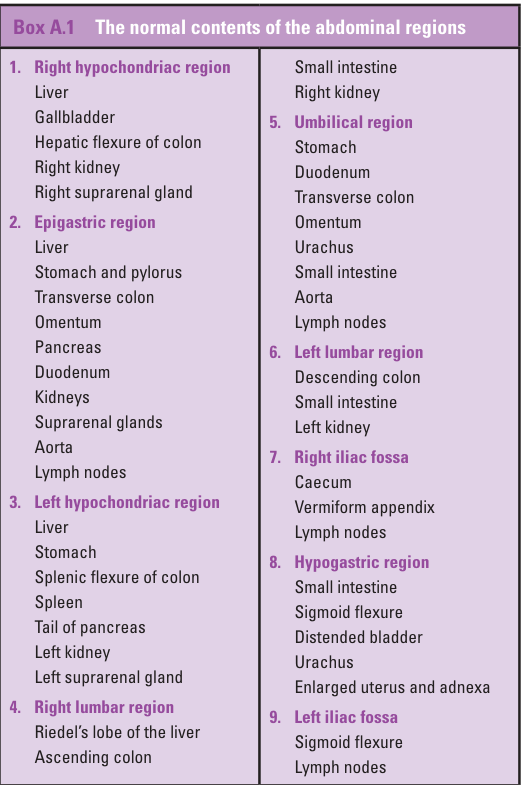
Epigastric region
Enlargement of the liver
may be felt in this area, and indeed it is
common to feel the normal liver in this region,
especially in infants and in adults with an
acute costal angle. The dilated stomach produced
by pyloric stenosis in either children or adults
may present as a visible swelling demonstrating
waves of peristalsis
traveling from left to
right. A succession splash is usually elicited.
Tumors of the stomach, apart from malignant
growth, are rare. A hundred years ago, a hair
ball or trichobezoar was frequently encountered
as an epigastric mass in hysterical girls who
chewed
and swallowed their hair, which then
formed an exact mold of the stomach. Hair balls
are only rarely encountered these days, and
modern textbooks hardly mention them; however,
as fashions and hair styles change, they may
reappear on the clinical scene. Other foreign
bodies are sometimes ingested by those with
learning difficulties and form a palpable mass.
In congenital pyloric stenosis, a tumor the size
of a small marble is palpable at the right
border of the right rectus.
The transverse
colon usually passes across the upper
part of
the umbilical area, and may be palpated when
it is the site of a carcinoma, when it is
impacted with faeces or when it is distended by
a large-bowel
obstruction placed distal to
it.
Swellings in connection with the omentum
may be due to tuberculous peritonitis or, more
commonly, due to infiltration with secondary
malignant deposits.
Swellings arising from
the pancreas push forward from the depths of the
abdominal cavity towards the epigastric and the
upper part of the umbilical areas, and present
themselves as vaguely palpable deeply seated
masses. They have the stomach, or the
stomach
and colon, in front of them and are fixed to the
posterior abdominal wall, thus moving only a
little on respiration. They may transmit a
non-expansile pulsation from the subjacent
aorta. Unless extremely large, such swellings
are resonant on percussion, due to the overlying
air-filled gut. A pancreatic swelling may be
carcinomatous, in which case wasting, anemia and
jaundice are likely to be observed. There may be
clay colored stools and dark urine, and it is
important to note that the onset of jaundice is
frequently preceded by deeply placed abdominal
pain, or pain in the back.
Glycosuria of
recent origin in an elderly patient also raises
suspicion of a pancreatic carcinoma. In about
half of the patients with jaundice due to
carcinomatous obstruction, the gallbladder is
palpably distended (Courvoisier's law).
Occasionally, the mass may result from chronic
pancreatitis; the swollen pancreas of acute
pancreatitis has only exceptionally been
palpated before laparotomy.
Pancreatic cysts are the pancreatic swellings
that are most commonly palpable. Only 20 percent
are true cysts; these are either single or
multiple retention cysts that usually result
from chronic pancreatitis, neoplastic cysts
(cystadenoma and cystadeno-carcinoma) and the
rare congenital polycystic disease of the
pancreas and hydatid cyst of the pancreas. Far
more often, the cysts are not in the pancreas
itself but comprise a collection
of fluid
sealed off in the lesser sac due to closure of
the foramen of Winslow (pseudocyst of the
pancreas).
This may occur after trauma to the
pancreas, following acute pancreatitis or, much
less commonly, resulting from perforation of a
posterior gastric ulcer. They may reach an
enormous size and fill the entire upper part of
the abdomen.
Retroperitoneal cysts are rare.
The majority arise from remnants of the
mesonephric (Wolffian) duct and occur in adult
women. Others are teratomatous, lymphangiomatous
or dermoid.
Retroperitoneal tumors (apart
from those arising in the pancreas, suprarenal
gland or kidney) originate in the mesenchymal
tissues, the sympathetic chain and the
para-aortic lymph nodes.
Swellings in connection with the duodenum are
exceedingly rare. They may result from an
inflammatory mass developing around a
penetrating duodenal ulcer, or be due to a
duodenal malignant tumor, but the latter is a
pathological curiosity. Those in connection with
the kidneys and suprarenal glands are found in
the epigastrium only if very large. Their
diagnosis is considered below.
Enlargement of
the spleen may bring its anterior edge into the
epigastric area; a splenic swelling always lies
in contact with the anterior wall of the
abdomen.
Lymph nodes, which are numerous in
the para-aortic retroperitoneal tissues and in
the mesentery, may become palpable in
reticuloses, tuberculous peritonitis, or
malignant disease as nodulated chains or masses.
Left hypochondriac region
An abnormal lobe
or a tumor in the left lobe of the liver may
appear as a superficial tumor in this area. Much
of the stomach normally lies in the left
hypochondrium; the diagnosis of gastric swelling
has been considered above, and a gastric tumor
is commonly felt in this region. On physical
signs alone, it must be differentiated from a
swelling of the adjacent spleen. A barium-meal
X-ray examination, ultrasound or computed
tomography (CT) scan help considerably in
differentiating between a gastric and
a
splenic swelling.
The diagnosis of a tumor of
the splenic flexure of the colon, whether
scybalous or malignant, is arrived at in the
same way as in the case of a tumor of the
hepatic flexure or transverse colon. The
distinguishing features are that the spleen
comes down from under the left costal margin in
direct contact with the anterior abdominal wall
(and is therefore dull on percussion), descends
on inspiration and has a smooth surface, and a
notch may be palpable on its inner margin. A
splenic swelling may be identified on a plain
X-ray of the abdomen and differentiated from a
renal mass by means of pyelography. A barium
meal examination may show displacement and
indentation of the adjacent stomach.
Ultrasound or CT scan will clinch the diagnosis.
Tumors of the pancreas may project into the left
hypochondrium, as may retroperitoneal tumors and
cysts. Tumors of the left kidney and suprarenal
gland have the stomach and colon in front of
them and therefore, unless extremely large, are
resonant on percussion.
Since they arise in
the loin, these masses can usually be balloted
by bimanual palpation.
Right lumbar region
Occasionally, a
congenital projection of the liver, known as
Riedel's lobe, may appear as a superficial tumor
continuous with the liver above it in this zone.
It may be mistaken for a dilated gallbladder.
The ascending colon may be palpable due to
contained faecal masses, owing to thickening as
a result of long-standing colitis, Crohn's
disease or hyperplastic tuberculosis, or due to
malignant disease.
The ascending colon can be
felt in acute or chronic ileocaecal and
ileocolic intussusception as a sausage shaped
tumor, at first situated in the right flank,
then moving across the abdomen above the
umbilicus and finally down the left flank into
the pelvis. The
vast majority of these cases
occur in infants or young children, usually aged
between 3 and 12 months.
Boys are affected
twice as often as girls. The history is of
paroxysms of abdominal colic typified by
screaming and pallor. There is vomiting and
usually the passage of blood and mucus per
rectum, giving the characteristic 'redcurrant
jelly stool'. A rectal examination almost always
reveals this typical feature, and rarely the tip
of the intussusception can be felt. In infants,
there
is usually no obvious cause, but the
mesenteric lymph nodes in these cases are
invariably enlarged. In adults, a polyp,
carcinoma or an inverted Meckel's diverticulum
may form the apex of the intussusception.
Tumours in connection with the right kidney and
suprarenal gland usually appear deep down in
this region, having the ascending colon and
small intestine in front of them. They can be
lifted forward en masse from behind by a hand
placed at the back of the loin and thus palpated
bimanually. The lower pole of the right kidney
can be felt in some normal persons on deep
abdominal palpation, especially in thin females.
When abnormally low and mobile, the whole of the
otherwise normal kidney may be palpable. Its
shape and consistency are characteristic. Renal
swellings move on respiration and, unless very
large, are resonant on percussion due to the
anteriorly related gut. However, Riedel's lobe
of the liver, an enlarged gallbladder, masses in
the ascending colon and secondary deposits in
the omentum have all been mistaken for it,
although they are more superficially placed and
lie in contact with the anterior abdominal wall.
Other wandering
masses, for example those
arising from the ovary, Fallopian tube and
mesentery, as well as hydatid cysts, are all
liable to the same error of identification.
Imaging by means of ultrasound or CT scanning is
invaluable in assisting with the differential
diagnosis.
Umbilical region
The grossly dilated
stomach resulting from long-standing pyloric
obstruction may occupy the umbilical region;
indeed, it may descend below it down into the
pelvis.
Tumors in connection with the
transverse colon have been considered in
'Epigastric region' and 'Right lumbar region',
above.
Tumors in connection with the omentum
are common in this region; those arising from
the small intestine are much rarer, although the
thickened small bowel in Crohn's disease may
form a palpable mass.
Swellings arising from
the kidneys, suprarenal glands, pancreas,
retroperitoneal tissues, para-aortic nodes and
mesentery may all present themselves in the
deeper parts of the umbilical region, usually as
more or less fixed masses arising from or
connected with the posterior wall of the
abdomen.
The aorta bifurcates 1 cm below and
to the left of the umbilicus in the supracristal
plane. Above (at the level of the fourth lumbar
vertebrae). In thin patients, pulsation of the
normal aorta can often be felt and indeed seen
in this region, and may lead to the incorrect
diagnosis of an abdominal aneurysm. Careful
examination, however, will show that this
pulsation is no more than a throbbing, an
up-and-down movement, and is not laterally
expansive.
Aneurysm of the abdominal aorta
forms an expansile mass situated above the
umbilicus itself, and it may be accompanied by
pain in the back from erosion of the bodies of
the lumbar vertebrae. Often, X-rays of the
abdomen in such cases will reveal calcification
in the aneurysmal wall. Ultrasound and CT enable
accurate delineation of the size and extent of
the aneurysm.
These methods are also valuable
in the visualization of the other
retroperitoneal masses enumerated above.
Left lumbar region
An enlarged spleen (see
'Left hypochondriac region', above) may protrude
into this area. It forms a firm mass that is in
contact with the abdominal wall, and its
dullness to percussion continues with its
thoracic dullness, which extends back up into
the axilla along the line of the ninth or tenth
ribs. Tumors in connection with the right
kidney, the right suprarenal gland and the
descending colon give rise to features similar
to those considered in 'Left hypochondriac
region', above.
Right iliac fossa
An inflammatory mass in
this region is most commonly associated with an
appendix abscess.
Less commonly, there may be
a paracaecal abscess in relation to a perforated
carcinoma of the caecum, or a solitary caecal
benign ulcer. A pyosalpinx may result from
salpingitis and, rarely, inflammatory swellings
may arise in connection with suppurating iliac
lymph nodes or a psoas abscess.
An important
differential diagnosis is between an appendix
mass and a carcinoma of the caecum. In the
former, there is usually a preceding episode of
an acute abdominal pain, typical of
appendicitis, with fever and leucocytosis. The
inflammatory mass subsides progressively over
2–3 weeks, and the occult blood test
in the
stools is negative. A carcinoma of the caecum
may be suspected if there is a preceding history
of bowel disturbance in a middle-aged or elderly
patient, if the mass fails to resolve rapidly
and if the occult blood test in the stools is
repeatedly positive. If there is any clinical
doubt, a barium enema X-ray examination should
be carried out and, if necessary, resort made to
laparotomy.
It is not at all rare for a soft
'squelchy' caecum to be palpable in a perfectly
normal thin female subject.
Occasionally, a
grossly distended gallbladder may project down
as far as the right iliac fossa, and a low-lying
kidney may form a palpable mass in this region.
Rarely, an ectopic kidney may be felt in one or
the other iliac fossa and, these days, a
transplanted kidney may be palpated at this
site. An ovarian tumor or cyst or a pedunculated
fibroid of the uterus may project into this
area.
Hypogastric region
The most common mass to
be felt in this region, after the pregnant
uterus, is the distended bladder. This may reach
as high as, or slightly above, the umbilicus.
Not uncommonly, this midline structure tilts
over to one or the other side. A distended
bladder has been tapped as ascites, operated
upon as an ovarian cyst or a fibroid, or
mistaken for the pregnant uterus. No diagnostic
opinion should be advanced, and no operative
procedure undertaken respecting a tumor in this
situation, until the bladder has been
emptied, either by voluntary micturition or by
the passage of a catheter.
Abdominal
swellings arising from the uterus, ovaries,
Fallopian tubes and uterine ligaments may all
rise up out of the pelvis and present themselves
as swellings in this region; as they grow
larger, they may be spread into any part of the
abdomen. While they remain comparatively small
and are manifestly connected with some
intrapelvic organ, their origin is not difficult
to determine.
However, when they have
extended into the abdomen or have acquired a
long pedicle, or have become fixed by adhesions
to some distant part of the abdominal wall or to
some other viscus, these pelvic tumors may give
rise to signs and symptoms that bear no relation
to pelvic disease. In such cases, they may only
be correctly diagnosed at laparotomy. The
discerning clinician will always remember the
possibility of pregnancy in every female patient
between menarche and menopause. The diagnosis is
confirmed by the urinary pregnancy test
(positive beta human
chorionic gonadotrophin
(hCG)) and, if necessary, by pelvic
ultrasonography.
Tumors of ileal Crohn's
disease arising in the small intestine may be
felt in the hypogastric area.
The urachus is
a fibrous cord running in the middle line in
front of the peritoneum from the fundus of the
bladder to the umbilicus. Occasionally, it
becomes the seat of cyst formation, more often
in women than in men. The urachal cyst is a
rounded tumor lying
between the umbilicus and
the pubic symphysis, which occasionally becomes
infected.
Left iliac fossa
The pelvic colon can
often be felt in normal subjects as a tube-like
cord, either when empty and in spasm, or else
when distended with faecal masses. The region is
a common site for carcinoma of the colon, and
there are usually symptoms of chronic intestinal
obstruction, or bowel disturbance with the
passage of blood and mucus in the stools. It is
clinically impossible to differentiate between
such a mass and that associated with
diverticular disease of the sigmoid colon.
Similarly, a paracolic abscess in this region
may equally well be associated with suppuration
of an inflamed colonic diverticulum or a
perforating carcinoma. Rarely, such an abscess
may be due to perforation of the tip of a long
appendix passing over the left iliac fossa, or
as an extreme rarity due to local perforation of
a left-sided appendix in transposition of
the
viscera. The diagnosis of this would be
suggested by finding the cardiac apex beat to
lie on the right side.
Please see also our Toxilact data base which is in the following language versions:
Toxilact Deutsche Sprachversion
Toxilact Nederlandstalige versie
Toxilakt έκδοση στην ελληνική γλώσσα
Toxilact English language version
Toxilact magyar nyelvű változat
Toxilact versione in lingua italiana
Toxilact polska wersja językowa
Detailed medical information on more common causes of acute abdomen
Intestinal Pain
Acute Appendicitis
Peritoneal Pain
Pain from Vascular Causes
Retroperitoneal Pain
Abdominal Pain from Intoxication
Toxicological risk during lactation
Toxicological lactation category I - the drug and/or its metabolites are either not eliminated through breast milk or are not toxic to the newborn and cannot lead to the development of absolutely any toxic reactions and adverse consequences for his health in the near and long term. Breast-feeding does not need to be discontinued while taking a given drug that falls into this toxicological lactation category.
Toxicological lactation category II - the drug and its metabolites are also eliminated through breast milk, but the plasma:milk ratio is very low and/or the excreted amounts cannot generate toxic reactions in the newborn due to various reasons, including degradation of the drug in the acid pool of the stomach of the newborn. Breastfeeding does not need to be discontinued while taking this medicine.
Toxicological lactation category III - the drug and/or its metabolites generate in breast milk equal to plasma concentrations or higher, and therefore the possible development of toxic reactions in the newborn can be expected. Breastfeeding should be discontinued for the period corresponding to the complete elimination of the drug or its metabolites from the mother's plasma.
Toxicological lactation category IV - the drug and/or its metabolites generate a plasma:milk ratio of 1:1 or higher and/or have a highly toxic profile for both the mother and the newborn, therefore their administration is incompatible with breastfeeding and it should to stop completely, and not just for the period of taking the drug, or to look for a less toxic therapeutic alternative.