Content
The content of medical knowledge in this section of the site of the Lactology Foundation is intended for the practical needs of doctors, pharmacists and students in these specialties. It is more than reasonable to consult other authoritative medical sources before using our medical knowledge.
- Pulmonology
- Cardiology
- Nephrology
- Emergency medicine
- Gastroenterology
- Hematology
- Oncology
- Rheumagology
- Allergology
- Neurology and Neurosurgery
- Endocrinology
- Pharmacotherapy and other medical knowledge
ABDOMINAL RIGIDITY
Rigidity of the abdomen is a sign of utmost importance, since in most cases it indicates serious intra-abdominal mischief requiring immediate operation.
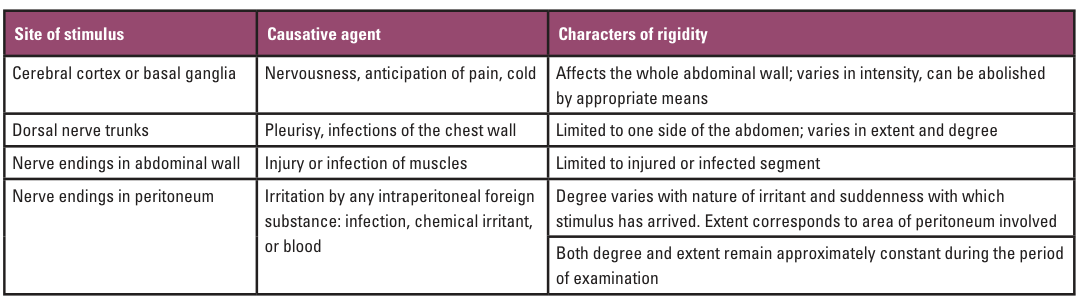
It is the expression of a state of tonic
contraction in the muscles of the abdominal
wall. The responsible stimulus may be in the
brain or basal ganglia, or in the territory of
the six lower dorsal nerves that supply the
abdominal wall. The extent of the rigidity will
depend on the number of nerves involved, and its
degree on the nature and duration of the
stimulus.
The analysis in the table below may
be considered.
The patient should be examined
lying on the back with the whole abdomen and
lower thorax exposed, but with the shoulders and
legs well covered. The room must be warm. The
examiner, seated on a level with the patient,
should first watch the abdomen to see whether it
moves with respiration or not, and whether one
part moves more than another; at the same time,
he or she may observe other things that will
help in the diagnosis, such as asymmetry of the
two sides, local swelling, or the movement of
coils of bowel.
While watching – and later when examining –
the examiner should engage the patient in
conversation, encouraging him to talk in order
to allay nervousness and to remove any part of
the rigidity that is due to a voluntary
contraction. Some nervous patients – especially
if the room is cold – hold their abdomens
intensely rigid, and can be induced to relax
only after gentle persuasion; a request to take
a few deep breaths, or to draw the knees up and
keep the mouth open, will often help.
During
this preliminary examination, one (well warmed)
hand may be laid gently on the abdomen and
passed over its surface with a light touch that
cannot possibly hurt; this maneuver will help to
allay the patient's anxiety still further and
give the examiner an idea of the extent,
intensity and constancy of the rigidity to be
investigated later in more detail.
For a more exact examination, the observer should sit at the patient's side facing their head, and place both hands on the abdomen, examining comparable areas of both sides, simultaneously, and taking in turn the epigastrium, right and left hypochondria, umbilical region, both flanks as far back as the erector spinae (as the rigidity of a retrocaecal appendix may only affect the posterior part of the abdominal wall), the hypogastrium and both iliac fossae. First, the whole hand should be applied with light pressure; next, the fingers held flat should be pressed more firmly to estimate the extent of the rigidity and to discover deep tenderness; last, a detailed examination may be made in suspected areas with the firm pressure of one or two fingers. Evidence is not complete without percussion and auscultation. A rectal examination is indispensable.
After a leisurely examination with warm hands
in a warm room, during which the physician has
also been able to sum up the patient, their
temperament, and whether they are really ill or
not, the rigidity of anxiety or cold will have
been dispelled or recognized .
The abdominal
rigidity due to a lesion in the chest or chest
wall usually involves a wide area limited to one
side – a distribution most unusual with
intra-abdominal mischief, which, if it has
spread widely but not everywhere, tends to be
limited to the upper or lower half. The extent
and degree of rigidity in chest affections also
vary widely during examination. Other things
such as a flushed face, rapid respiration,
movement of the alae nasi, or a temperature of
more than 39 °C (102 °F) may suggest that the
lesion is not abdominal, and a friction rub may
be felt or heard in the chest.
Auscultation
and rectal examination dispel any remaining
doubts, as in chest conditions peristaltic
sounds remain normal and there is no tenderness
in Douglas's pouch.
Examination of the blood
may show a high leucocytosis (up to 30,000 or
40,000 per mm3), whereas in peritonitis the
count is rarely over 12,000 per mm3.
Chest
X-rays (including a lateral film) will
demonstrate the intrathoracic lesion.
Injuries of the abdominal wall, and particularly
those caused by run-over accidents, lead to very
marked rigidity of the injured segment. Here,
the rigidity is not necessary to establish a
diagnosis, as the injury is already known, but
its degree and extent should be carefully noted.
There must always be a doubt as
to whether
the abdominal viscera are damaged as well as the
walls, and this point can only be settled by
careful observation. The patient is put to bed
and kept warm, the pulse is charted every 15
minutes, and the abdomen is re-examined from
time to time.
In the case of a mere
contusion, the collapse will soon disappear, the
abdomen will become less rigid, and the pulse
rate will fall. If the contents of a hollow
viscus have escaped, rigidity will extend beyond
the area of the damaged muscles, and the signs
of peritonitis will develop rapidly. An X-ray of
the abdomen, in the
erect position, will
demonstrate free gas beneath the diaphragm. If
there is internal bleeding (e.g. from a ruptured
spleen or liver), there is pallor and
progressive elevation of the pulse, together
with a falling blood pressure. Dullness in the
flanks (especially on the left side, in rupture
of the spleen) is often detected, as blood
collects in the paracolic gutters.
PERITONITIS
The most common and the most
important cause of general abdominal rigidity is
peritonitis, and it is a safe rule when meeting
true rigidity to diagnose peritonitis until it
can be excluded. Actually, rigidity means no
more than that the parietal peritoneum lining
the abdominal cavity is in contact with
something different from the smooth surfaces
that are its normal environment. The presence of
rigidity therefore announces a change in the
coelomic cavity that is probably infectious in
origin.
When gallstone colic is followed by
rigidity of the right rectus muscle, it means
not only that a stone is blocking the cystic
duct, but also that the wall of the gallbladder
is inflamed. Intestinal obstruction of
mechanical origin (such as that due to a band or
adhesion) gives colic referred to the umbilicus
but no guarding of the muscles; local rigidity
accompanying the clinical picture of intestinal
obstruction indicates that there is also a local
inflammatory focus such as a strangulated loop
of bowel, while a more diffuse rigidity suggests
changes such as thrombosis of the
superior
mesenteric artery, affecting a large segment of
bowel. In appendicitis, rigidity denotes that
the infection has spread beyond the coats of the
appendix.
The degree of rigidity varies with
the nature of the irritant, the rapidity with
which the peritoneum is attacked, and the area
involved. At one extreme is the rigidity of a
gastric or duodenal perforation, where the
abdomen is suddenly flooded with gastric
contents. Here, the whole abdominal wall is
fixed in a contraction that can best be
described as board-like: there is no respiratory
movement, and no yielding to the firmest
pressure. At the other extreme is the relatively
minor degree of rigidity that accompanies
the
presence of small amounts of blood or urine in
the peritoneal cavity; there is perhaps only a
slightly increased resistance when the hands are
pressed on the abdomen. Perforation of a gastric
or duodenal ulcer produces the most intense
rigidity; the escape of
amylase in acute
pancreatitis leads to less rigidity, and the
escape of other sterile fluids, urine for
instance, or blood, still less. Bacterial
invasion of the peritoneum produces marked
rigidity.
The degree of muscle contraction also changes
during the development of a case. The board-like
abdominal wall of a perforation is considerably
softer after 3–4 hours when the peritoneum has
recovered from the shock of the first insult.
The slight resistance apparent when sterile
urine escapes from a ruptured bladder rapidly
increases as infection occurs.
The extent of
the rigidity usually corresponds to the area of
peritoneum affected. The entire abdomen may be
rigid, or it may affect only the upper or lower
part, one side or a restricted part. Total
rigidity should mean a total peritonitis, but
because the peritoneum reacts immediately to
invasion by forming adhesions that localize the
mischief, a general peritonitis is only seen
when an irritant or infected fluid is suddenly
discharged in large quantities – as in duodenal
perforation, pancreatitis or the bursting of a
large abscess or distended viscus – or when the
infection is brought by the bloodstream and
reaches all parts
simultaneously.
Occasionally, and particularly in children, the
reaction to a sudden infection may be excessive
and the muscles contract over a wide area in
response to a purely local infection, for
instance of the appendix, although this
exaggerated response
quickly disappears.
Conversely, the aged patient – with atrophic
abdominal muscles – may exhibit only slight
rigidity, even in generalized peritonitis.
Local peritonitis starts around some site of
infection, and as it spreads it is guided by
certain peritoneal watersheds, of which the most
important is the attachment of the great omentum
to the transverse colon, dividing the abdomen
into supra- and infracolic
compartments:
rigidity accompanies the infection.
Thus,
localized rigidity is found over any inflamed
organ, and as the infection and the guarding
spread, they tend to involve the upper or the
lower half of the abdomen as a whole. When we
have mapped out the extent of the rigidity, we
should – from a knowledge of the organs at that
site and of the watersheds that
guide the
spread of infection – be able, in conjunction
with the history, to make a diagnosis.
The influence of natural subdivisions in
guiding intraperitoneal extension must always be
taken into account. Infections in the right
supracolic compartment tend to pass down between
the ascending colon and the right abdominal
wall, while one in the pelvis is guided by the
pelvic mesocolon to the left side of the abdomen
as it ascends. Thus, rigidity in the right iliac
fossa may indicate a leaking duodenal ulcer, and
rigidity in the left may be due to a pelvic
appendix.
Since the diagnosis of peritonitis
in most cases means immediate operation, every
effort must be made to confirm the diagnosis,
particularly by the simple tests of percussion,
auscultation and rectal examination. Percussion
may reveal the outline of some dilated hollow
organ, such as the caecum; it may disclose free
gas that has escaped from a perforation as a
shifting circle of resonance or a tympanitic
note where liver dullness should be; it may map
out an abnormal area of dullness where there is
an abscess or a collection of blood; or it may
indicate
free fluid in the peritoneum.
Auscultation is even more important, as
peristalsis ceases with peritonitis: in a normal
abdomen, peristaltic sounds can be heard every
4–10 seconds; in obstruction, they are increased
in loudness, pitch and frequency; but in
peritonitis, there is complete silence. Rectal
examination almost always reveals tenderness
when there is intra-abdominal infection, even if
it is distant and localized.
Other signs must
be mentioned: the patient lies still, sometimes
with the knees drawn up, and resists
interference. The abdomen gradually becomes
distended, tense and tympanitic. The tongue is
brown and dry. Vomiting is to be expected at the
onset of any abdominal catastrophe, but it
usually ceases, except in intestinal
obstruction. With advancing peritonitis, it
reappears, and the vomit becomes first
bile-stained, later brownish and
faecal-smelling, and is allowed to dribble from
the corner of the mouth in contrast to the
projectile vomiting of obstruction. There may be
diarrhea at
first, but absolute constipation
soon succeeds it. The temperature tends to fall;
the pulse is small and rapid, rising
progressively. In late stages, the sunken
cheeks, wide eyes and anxious expression of the
patient form a characteristic feature – the
Hippocratic facies.
These signs are
indications of a peritonitis discovered too
late, and are the heralds of approaching death.
Abdominal rigidity, abdominal silence, rectal
tenderness and a rising pulse are a tetrad that
calls for immediate definitive treatment.
A
more detailed diagnosis is usually possible when
the history and other signs are taken together,
but a consideration of all the alternatives is
out of the question in this section. Abdominal
paracentesis with a fine needle may clinch the
presence of pus, blood or urine in the
peritoneal cavity, but a false-negative tap may
delay rather than aid diagnosis. A list of the
more common conditions associated with rigidity
may, however, help the inquiry:
• Stomach or duodenum
– Perforation of
peptic ulcer
• Gallbladder
– Acute
cholecystitis
– Rupture of the gallbladder
• Pancreas
– Acute pancreatitis
• Small
intestine
– Strangulation of a loop
–
Traumatic perforation
– Mesenteric vascular
thrombosis or embolism
– Meckel's
diverticulitis
– Acute ileitis
• Large
intestine
– Appendicitis
– Volvulus
–
Diverticulitis with perforation
• Peritoneum
– Acute blood-borne peritonitis
⚬
Streptococcal
⚬ Pneumococcal
⚬ Gonococcal
• Female reproductive organs
– Twisted
ovarian cyst
– Ruptured ectopic pregnancy
– Acute salpingitis
– Torsion or red
degeneration of a fibroid
– Perforation of
the uterus or posterior fornix of vagina in
attempted abortion
• Spleen and/or liver
–
Traumatic rupture
• Aorta
– Ruptured
aneurysm
Perforation of a peptic ulcer is
characterized by the most sudden onset, the
worst agony and the most extreme abdominal
rigidity that the physician is ever likely to
see. Radiation of pain to the right shoulder tip
(referred pain from diaphragmatic irritation)
may be experienced. Immediately afterwards, the
patient is motionless and speechless, in a state
of obvious collapse. A few hours later, pain,
rigidity and shock have all diminished, and only
the dramatic history of sudden onset and
persistent abdominal and rectal tenderness may
remain to indicate the seriousness of the
condition.
Acute pancreatitis is rarely
accompanied by the severe pain described in
textbooks, or indeed by pain as bad as that of
gallstone colic. The abdominal rigidity is more
marked in the upper abdomen but is not profound.
On the other hand, the patient shows a degree of
toxaemia out of all proportion to the physical
signs in the abdomen. The diagnosis is confirmed
by a considerable rise in the serum amylase. A
ruptured ectopic pregnancy may simulate a lower
abdominal peritonitis, but the signs of bleeding
predominate and rigidity is not well marked. If
the patient is a woman of child-bearing age who
is known to have missed a period, the onset of
abdominal pain and pallor suggest the diagnosis.
Extravasated blood will be felt in the pelvis,
together with acute tenderness on vaginal and
rectal examinations. The diagnosis is confirmed
by the urinary pregnancy test (positive beta
human chorionic gonadotrophin (hCG)) and, if
necessary, by pelvic ultrasonography.
Blue
discoloration of the skin around the umbilicus -
Cullen's sign - may be associated with rigidity.
This discoloration is due to extravasated blood
coming forward from the retroperitoneal space.
The sign is seen in ruptured kidney, leaking
abdominal aneurysm and acute pancreatitis.
Occasionally, it is seen in ruptured ectopic
pregnancy, when the blood gains entry to the
subperitoneal space through the broad ligament.
Although pancreatitis may produce this sign, it
is more common to see a green discoloration in
the loins (Grey Turner's sign).
Please see also our Toxilact data base which is in the following language versions:
Toxilact Deutsche Sprachversion
Toxilact Nederlandstalige versie
Toxilakt έκδοση στην ελληνική γλώσσα
Toxilact English language version
Toxilact magyar nyelvű változat
Toxilact versione in lingua italiana
Toxilact polska wersja językowa
Detailed medical information on more common causes of acute abdomen
Intestinal Pain
Acute Appendicitis
Peritoneal Pain
Pain from Vascular Causes
Retroperitoneal Pain
Abdominal Pain from Intoxication
Acute appendicitis in children
Toxicological risk during lactation
Toxicological lactation category I - the drug and/or its metabolites are either not eliminated through breast milk or are not toxic to the newborn and cannot lead to the development of absolutely any toxic reactions and adverse consequences for his health in the near and long term. Breast-feeding does not need to be discontinued while taking a given drug that falls into this toxicological lactation category.
Toxicological lactation category II - the drug and its metabolites are also eliminated through breast milk, but the plasma:milk ratio is very low and/or the excreted amounts cannot generate toxic reactions in the newborn due to various reasons, including degradation of the drug in the acid pool of the stomach of the newborn. Breastfeeding does not need to be discontinued while taking this medicine.
Toxicological lactation category III - the drug and/or its metabolites generate in breast milk equal to plasma concentrations or higher, and therefore the possible development of toxic reactions in the newborn can be expected. Breastfeeding should be discontinued for the period corresponding to the complete elimination of the drug or its metabolites from the mother's plasma.
Toxicological lactation category IV - the drug and/or its metabolites generate a plasma:milk ratio of 1:1 or higher and/or have a highly toxic profile for both the mother and the newborn, therefore their administration is incompatible with breastfeeding and it should to stop completely, and not just for the period of taking the drug, or to look for a less toxic therapeutic alternative.