Content
The content of medical knowledge in this section of the site of the Lactology Foundation is intended for the practical needs of doctors, pharmacists and students in these specialties. It is more than reasonable to consult other authoritative medical sources before using our medical knowledge.
- Pulmonology
- Cardiology
- Nephrology
- Emergency medicine
- Gastroenterology
- Hematology
- Oncology
- Rheumagology
- Allergology
- Neurology and Neurosurgery
- Endocrinology
- Pharmacotherapy and other medical knowledge
ABDOMINAL PULSATION
A pulsatile swelling in the
abdomen may be due to:
• A
prominent aorta – normal or
arteriosclerotic
• An abdominal
aortic aneurysm
• Transmission of
aortic pulsations through an
abdominal mass
• A pulsatile,
enlarged liver
PROMINENT AORTA
The pulsations of the
normal aorta may be felt in perfectly normal but
thin subjects along a line extending from the
xiphoid to the bifurcation of the aorta at the
level of the fourth lumbar vertebra. This is on
a line joining the iliac crests, about 2 cm
below and a little to the left of the umbilicus.
In the arteriosclerotic and hypertensive
subject, it may be difficult to decide whether
or not the aorta is merely thickened and
tortuous, or whether it is aneurysmal. If the
two index fingers are placed parallel, one on
either side of the aorta, the distance between
the fingers can be measured.
According to the
size of the patient, a gap of 2–3 cm between the
fingertips may be considered normal, but any
measurement above this is suspicious of
aneurysmal dilatation.
If in doubt,
visualization of the aorta by means of
ultrasound or computed tomography enables
accurate measurement of the aorta to be made.
ABDOMINAL AORTIC ANEURYSM
There is no
doubt that arteriosclerotic abdominal aneurysms
are becoming more frequently encountered, as is
the serious emergency of leakage or rupture of
such an aneurysm. The majority of patients are
aged more than 60 years, and the great majority
are men. The aneurysm may be entirely
symptomless or the patient may complain of
epigastric or central abdominal discomfort that
frequently radiates into the lumbar region.
Patients themselves may actually detect the
pulsating mass in the abdomen.
The pulsation
may be visible in the upper abdomen, above the
umbilicus, and – if large enough – may actually
appear as a pulsating mass. On palpation, the
aneurysm is a midline swelling that bulges over
to the left side, away from the adjacent
inferior vena cava. If the mass extends below
the level of the umbilicus, it suggests
involvement of the iliac arteries.
The
characteristic physical sign is that the mass
has an expansive pulsation. The index fingers
are placed on either side of the mass, which
enables the diameter to be assessed. If the
diameter is more than 3 cm, this certainly
suggests aneurysmal dilatation of the aorta; if
the diameter is above 5 cm, the clinical
diagnosis is
all but certain. Typically, the
fingers are pushed apart with each pulse, and
not up and down. The latter sign suggests
transmission of the pulsation.
Usually, the
aneurysm is resonant to percussion due to
overlying loops of intestine. However, an
extremely large aneurysm will displace the bowel
laterally to reach the anterior abdominal wall
and will then give a dull percussion note.
Auscultation may reveal bruits over the lower
extremity of the aneurysm. This suggests
turbulent flow of blood caused by relative
stenosis at the aortoiliac junctions.
Rectal
examination may reveal a pulsatile mass when one
or both of the internal iliac arteries are
involved in the aneurysmal process.
Leakage
or rupture of the aneurysm is an acute
abdominal emergency. The patient presents with
the features of massive blood loss (pale,
sweating,
clammy skin, a rapid pulse and low
blood pressure)
together with severe
abdominal pain, lumbar pain
and marked
abdominal tenderness and guarding.
Because of
the low blood pressure and the associated
peri-aneurysmal haematoma, as well as the
overlying one guarding, the aneurysm may be
quite difficult to
palpate and, unless sought
carefully, is easy enough
to miss.
The
diagnosis of aortic aneurysm is often readily
confirmed by means of a plain abdominal X-ray,
which frequently delineates the aneurysm because
of the associated calcification in its wall.
Typically, the aneurysm is seen to bulge over to
the left side of the abdomen. More accurately,
an ultrasound or computed tomogram of the
abdomen visualizes the aneurysm and enables its
length and diameter to be measured accurately.
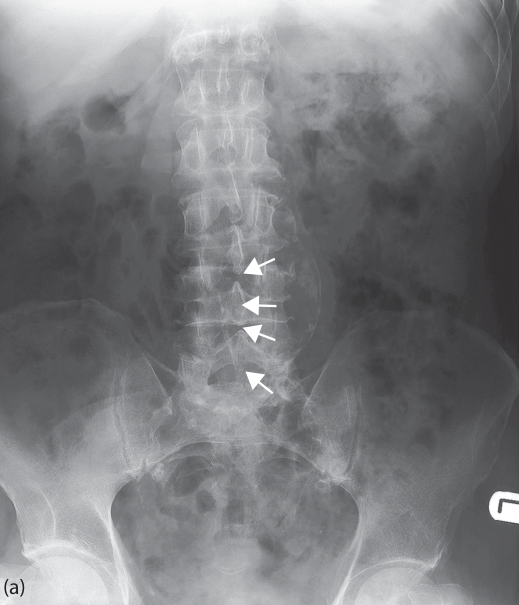
Plain X-ray of the abdomen, showing a large calcified aortic aneurysm (arrowed).
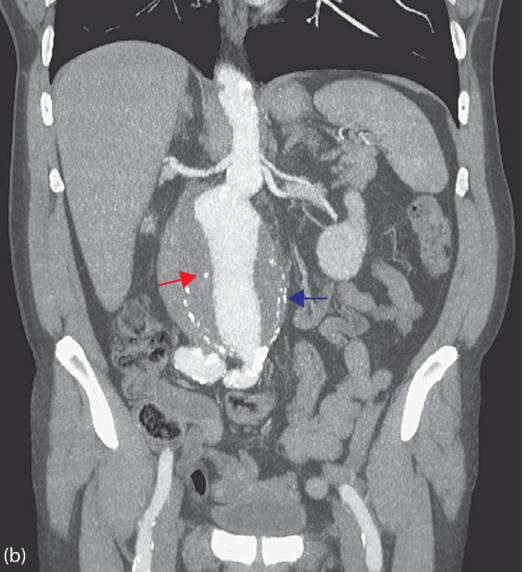
Coronal computed tomography image of an infrarenal aortic aneurysm with a calcified wall (blue arrow) and intraluminal thrombus (red arrow). The arteries have been enhanced by an intravenous injection of contrast.
TRANSMISSION OF AORTIC PULSATIONS THROUGH AN
ABDOMINAL MASS
A large intra-abdominal or
retroperitoneal solid mass, pressing against the
aorta, may exhibit transmitted aortic pulsation.
Typical examples are a large carcinoma of the
body of the stomach, a carcinoma or cyst of the
pancreas, and a large ovarian cyst. Indeed, when
the entire abdomen is filled by a cystic mass,
it may be quite difficult to distinguish between
such a mass and extensive ascites. Percussion,
of course, is helpful since ascites gives
dullness in the flanks as compared with the
central dullness of a large intra-abdominal
mass. The two index fingers, when placed on the
mass, will perceive that the pulsation is
transmitted directly forwards from the aorta and
is not expansive, as would be found in an
aneurysm.
PULSATILE LIVER
It is unlikely that an
enlarged pulsatile liver will be mistaken for
any other kind of pulsatile tumor.
It occurs
in cases of chronic failure of cardiac
compensation, generally from mitral stenosis or
tricuspid stenosis. There is associated
cyanosis, edema of the legs and ascites. It is
not, however, every liver which seems to pulsate
that really presents expansive pulsation. An
impression of pulsation may be given by the
movements transmitted directly to the liver by
the hypertrophied right heart.
Please see also our Toxilact data base which is in the following language versions:
Toxilact Deutsche Sprachversion
Toxilact Nederlandstalige versie
Toxilakt έκδοση στην ελληνική γλώσσα
Toxilact English language version
Toxilact magyar nyelvű változat
Toxilact versione in lingua italiana
Toxilact polska wersja językowa
Detailed medical information on more common causes of acute abdomen
Intestinal Pain
Acute Appendicitis
Peritoneal Pain
Pain from Vascular Causes
Retroperitoneal Pain
Abdominal Pain from Intoxication
Toxicological risk during lactation
Toxicological lactation category I - the drug and/or its metabolites are either not eliminated through breast milk or are not toxic to the newborn and cannot lead to the development of absolutely any toxic reactions and adverse consequences for his health in the near and long term. Breast-feeding does not need to be discontinued while taking a given drug that falls into this toxicological lactation category.
Toxicological lactation category II - the drug and its metabolites are also eliminated through breast milk, but the plasma:milk ratio is very low and/or the excreted amounts cannot generate toxic reactions in the newborn due to various reasons, including degradation of the drug in the acid pool of the stomach of the newborn. Breastfeeding does not need to be discontinued while taking this medicine.
Toxicological lactation category III - the drug and/or its metabolites generate in breast milk equal to plasma concentrations or higher, and therefore the possible development of toxic reactions in the newborn can be expected. Breastfeeding should be discontinued for the period corresponding to the complete elimination of the drug or its metabolites from the mother's plasma.
Toxicological lactation category IV - the drug and/or its metabolites generate a plasma:milk ratio of 1:1 or higher and/or have a highly toxic profile for both the mother and the newborn, therefore their administration is incompatible with breastfeeding and it should to stop completely, and not just for the period of taking the drug, or to look for a less toxic therapeutic alternative.