Content
The content of medical knowledge in this section of the site of the Lactology Foundation is intended for the practical needs of doctors, pharmacists and students in these specialties. It is more than reasonable to consult other authoritative medical sources before using our medical knowledge.
- Pulmonology
- Cardiology
- Nephrology
- Emergency medicine
- Gastroenterology
- Hematology
- Oncology
- Rheumagology
- Allergology
- Neurology and Neurosurgery
- Endocrinology
- Pharmacotherapy and other medical knowledge
Abdominal Pain from Intoxication
Severe colicky diffuse abdominal cramp pain occurs in lead poisoning. The abdomen may be tense but remains compressible and there is no particular pain upon palpation. There is no rebound tenderness. In principle, all heavy metals can cause abdominal pain. Abdominal pain associated with thallium poisoning is similar to that of lead poisoning and porphyria, which is characterized by persistent constipation and an intermittent pattern.
Porphyrias
Porphyria should be considered
in patients with unclear recurring abdominal
pain. A positive family history and intermittent
occurrence are typical. In some cases the pain
can be triggered by drugs and is associated with
neurological and dermatological manifestations
(photosensitivity). Abdominal colic due to
porphyria is frequently misinterpreted,
resulting in a surgical intervention.
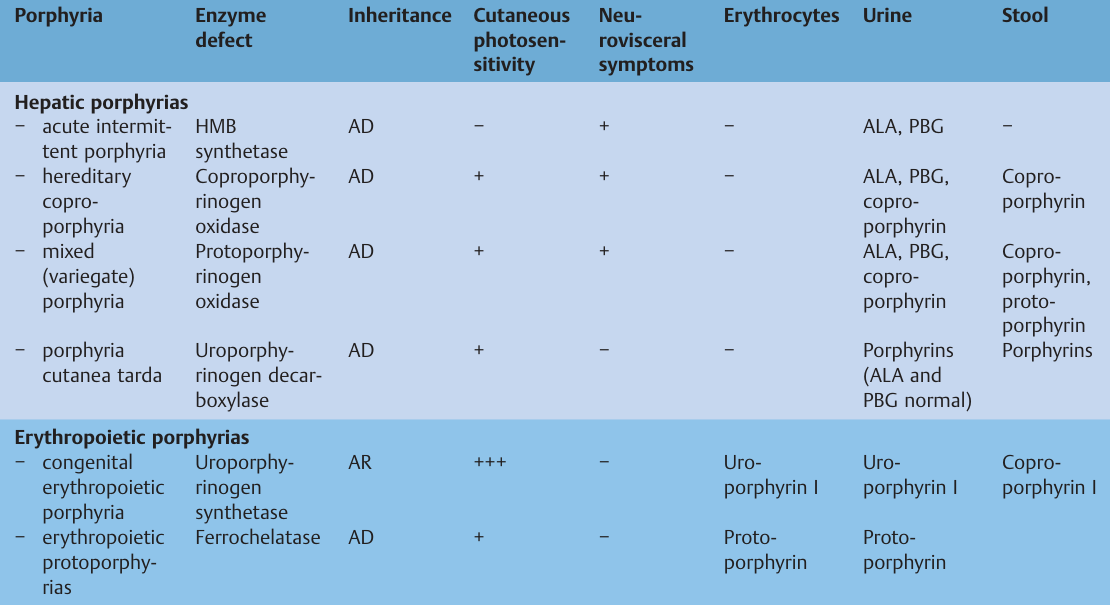
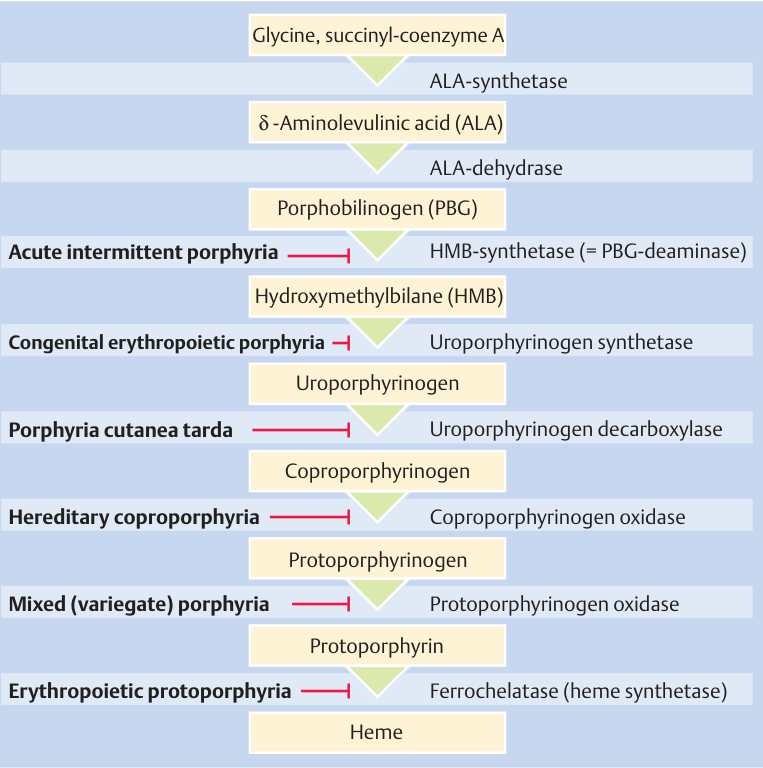
Pathogenesis
Porphyrias are hereditary
disorders of heme metabolism. Porphyrias are
classified according to the site of
overproduction and accumulation of porphyrin
precursors into hepatic and erythropoietic
forms. Similar abdominal colics are observed
with acute intermittent porphyria (AIP),
hereditary coproporphyria (HCP), and variegate
porphyria (VP). All three forms can be triggered
by drugs. Signs of cutaneous photosensitivity
are found with HCP, VP, porphyria cutanea tarda
(PCT), and the erythropoietic
porphyrias. In
recent years the enzyme defects and underlying
genetic mutations responsible for the various
forms of porphyria have been identified.
Hepatic Porphyrias
The
most important forms of hepatic porphyria are
AIP, HCP, VP, and PCT.
Acute Intermittent
Porphyria
AIP generally becomes symptomatic
in the third decade of life, very rarely before
puberty, and is uncommon after the age of 60.
The ratio of men to women affected is 2 : 3.
Abdominal colic (patients are frequently
subjected to laparotomy several times before
diagnosis ), often accompanied by constipation
or ileus, nausea, vomiting without
palpation-sensitive abdomen, motor paralysis as
part of a primarily peripheral neuropathy, and
cerebral symptoms characterize the variable
clinical picture. Often only a slight muscular
weakness can be noted. All muscles, including
the facial muscles, may be affected. Ascending
paralysis occurs. Affection of the respiratory
muscles may cause respiratory insufficiency.
Paresis may recede. Epileptiform attacks and
psychiatric symptoms (anxiety attacks,
sleeplessness, depression, hallucinations, etc.)
are not unusual. Additional symptoms are
tachycardia, hypertension, fever, and moderate
leukocytosis. Typically, acute attacks are
triggered by barbiturates and other drugs (e.
g., sulfonamides, pyrazolone, ergotamine
preparations, succinimide, carbamazepine).
Alcohol, weight-reduction diets, and endogenous
or exogenous sex hormones can also trigger an
episode. The urine excreted during an attack
darkens and does not
lighten after a few
hours, in contrast to normal urine with
urobilirubin. Increased excretion of
δ-aminolevulinic acid (ALA) and
porphyrobilinogen (PBG) in the urine during an
acute episode are diagnostic. Unlike HCP and VP,
porphyrin excreted in the stool in AIP is
generally normal.
In the latent stage
diagnosis can be made by the detection of
reduced hydroxymethylbilane (HMB) synthetase
activity in the erythrocytes.
Hereditary
Coproporphyria
Triggering factors, as well as
neurovisceral and other symptoms, correspond to
those of AIP. Skin photosensitivity is similar
to that of VP and PCT. The excretion of
coproporphyrin in urine and stool is increased
during acute attacks, but often also in the
interval. ALA and PBG excretion in the urine is
increased during the attacks.
Variegate
Porphyria
The incidence of VP among the white
population in South Africa is 0.3%, but it is
rare in the Western world. Triggering factors
and neurovisceral and other symptoms are similar
to those of AIP.
Cutaneous photosensitivity
is similar to that of HP and PCT. The excretion
of ALA, PBG, and coproporphyrin in urine and of
coproporphyrin and protoporphyrin in the stool
is increased.
Porphyria Cutanea Tarda
PCT
is the most common form of porphyria and is
observed almost exclusively in men. The skin
manifestations (photosensitivity) are dominant.
Neurological manifestations and abdominal pain
are not observed. Different types are
distinguished, but all have a defect of the
hepatic uroporphyrinogen decarboxylase in
common. Various factors can
contribute to
reduced enzyme activity, particularly alcohol
use, hepatic iron overload, and estrogens.
Chronic liver diseases (fatty liver, fibrosis,
cirrhosis) are frequent and may dominate the
clinical picture. Patients with PCT have an
increased risk of developing hepatocellular
carcinoma.
An association with chronic
hepatitis C has been described. Porphyrins in
the urine and stool are increased. ALA and PBG
excretion in the urine is typically normal.

Erythropoietic Porphyrias
The most important erythropoietic porphyrias are
congenital erythropoietic porphyria (CEP) and
erythropoietic protoporphyria (EPP).
Congenital Erythropoietic Porphyria
This is
an autosomal recessively inherited disease
characterized by hemolytic anemia, high-grade
photosensitivity of the skin, and accumulation
of the type I isomers of uroporphyrin and
coproporphyrin. Marked skin changes with
blisters, followed by scars and dystrophic
changes of body parts exposed to the light
dominate the clinical picture, and occur shortly
after birth. The red urine contains primarily
uroporphyrin I and somewhat less coproporphyrin
I. The ratio is reversed in the stool. ALA and
PBG excretion is normal. Hemolytic anemia with
ineffective erythropoiesis and splenomegaly are
typical.
Erythropoietic Protoporphyria
EPP
is the second most common form of porphyria
after PCT. It is an inherited autosomal dominant
disease caused by a defect of ferrochelatase.
Protoporphyrin accumulates in the erythrocytes
and in the plasma and is excreted in bile and
stool. The symptoms are generally mild,
transitory skin changes after exposure to
sunlight (itching, burning, reddening,
urticaria) but may vary from patient to patient
and during the course of the disease. Blisters
are rare compared with other porphyrias with
skin photosensitivity. Hemolysis or anemia is
generally not present or only mild. In some
patients the accumulation of protoporphyrin
causes chronic liver disease. Increased
protoporphyrin in the erythrocytes and proto-
porphyrin in the stool are diagnostic. The urine
is normal.
Lead Poisoning
Lead poisoning
causes a special form of porphyrinuria. In
children, encephalopathy is dominant, whereas in
adults colic and neuromuscular manifestations
predominate. The lead seam on the gums is also
typical. Lead anemia is due to hemolysis, caused
by direct damage of erythrocytes and inhibition
of erythropoiesis. The relative involvement of
these two mechanisms is variable.
Reticulocytosis can be marked or absent. The
characteristic basophile punctation of the
erythrocytes corresponds to altered ribosomes.
Longer lasting subclinical intoxication can
cause deficiencies in intellectual development
in children and renal insufficiency in adults.
Lead inhibits heme synthesis at various times
levels (ALA synthetase, ALA dehydrase,
ferrochelatase). Increased ALA excretion is a
typical symptom. Copro porphyrin III excretion
is also increased. PBG excretion is generally
normal, or at most moderately increased.
Erythrocyte protoporphyrin is markedly
increased. Diagnosis is confirmed by an
increased lead level in the blood or an
increased lead excretion in the urine and stool.
Abdominal Pain in Other Medical Diseases
Abdominal pain occurs not only with local
diseases, but can also be the leading symptom of
many general diseases. The most frequent general
diseases that must be considered here are listed
below.
Metabolic and Endocrine Diseases
Diabetic precoma is frequently accompanied by
severe abdominal pain primarily localized in the
epigastric region, and accompanied by severe
vomiting. The differential diagnoses, therefore,
include perforated ulcer, cholecystitis, and
acute pancreatitis. Leukocytosis is common in
all these conditions. Patients with acute
endocrinologic disorders also frequently
experience abdominal cramps, often associated
with vomiting or diarrhea. In particular,
thyreotoxicosis, acute hyperparathyroidism, and
pheochromocytoma must be considered in the
differential diag-
nosis of abdominal cramps.
Very severe abdominal pain can also be observed
in familiar hyperlipidemia (type I, IV, V). If
hyperlipidemia is associated with a surgical
abdomen, the clinician must search for
additional signs: xanthomas, lipemic retinitis,
and rarely hepatosplenomegaly. Triglycerides are
significantly increased in serum, giving rise to
its milky appearance. Transient hyperlipidemia
in alcoholics associated
with jaundice and
hemolytic anemia - Zieve syndrome; may also lead
to severe epigastric pain.
Similar acute pain
is observed with alcoholic hepatitis.
Chest Diseases
Pain
radiating to the epigastric region is frequent
with myocardial infarction, particularly with
posterior myocardial infarction.
The
diagnosis is straightforward if chest pain is
concomitant. It is often overlooked, however, if
the pain is exclusively localized in the
epigastric region. ECG and laboratory tests
usually confirm the diagnosis.
Acute
pulmonary diseases, particularly pleuritis,
pneumonia, spontaneous pneumothorax, and
pulmonary embolism (infarction), can cause
abdominal pain. A chest x-ray is usually
diagnostic.
Small amounts of free air under
the diaphragm can be better detected in the
chest x-ray than in the abdominal view.
Liver
Diseases
Severe epigastric pain is observed
occasionally with various liver diseases,
particularly with acute right-sided heart
failure, alcoholic hepatitis, and neoplasias of
the liver.
Collagen Diseases
These can
cause abdominal pain by involving small and
medium-sized vessels. Vascular occlusion in
systemic lupus erythematosus or panarteritis
nodosa results in infarctions (e.g., splenic,
pancreatic) or ulcers in the gastrointestinal
tract, and corresponding complications (e.g.,
hemorrhage, perforation, stenosis). Abdominal
pain is also observed with various rheu-
matic-allergic diseases, such as
Henoch−Schönlein purpura and in Behçet syndrome.
Indeterminate gastrointestinal complaints and
signs of ileus, perforation, and peritonitis may
be observed primarily in young men with
Köhlmeier−Degos syndrome. Diagnostic hallmarks
are skin changes (malignant atrophic papulosis)
that usually precede gastrointestinal symptoms.
The reddish papillae appear on the trunk and the
proximal parts of the extremities over days to
weeks, they become pale in the center and are
surrounded by a slightly raised violet ring with
telangiectasia. The cause of the underlying
obliterating endothelial reaction of the small
arteries, arterioles, and veins is unknown. This
rare disease is usually lethal.
Hematologic Diseases
Abdominal pain in patients with primary
hematologic diseases is often caused by
complications such as cholelithiasis in
congenital spherocytosis, nephrolithiasis in
leukemia, splenic infarction in
polycythemia,
retroperitoneal or intestinal hematoma in
coagulation disorders.
Allergic Diseases
With severe allergic reactions (e.g., serum
sickness) abdominal pain may precede other
allergic symptoms (e.g., skin changes) in the
form of severe continuous pain in the kidney
region or as cramplike pain in the epigastric
and hypogastric regions.
Infectious Diseases
Abdominal symptoms are frequent in most acute
infections and range from loss of appetite to
severe pain. The pain associated with Bornholm
disease may occasionally be localized primarily
in the abdominal region. Abdominal pain may
occur in various parasitic infections,
particularly trichinosis, ascaridiasis,
trichiuriasis, and tapeworm infections.
Neurogenic Abdominal Pain
Abdominal pain may also be a manifestation of a
neurological disease. The following syndromes
should be considered:
➤ tabes dorsalis
(tabetic neurosyphilis)
➤ intercostal
neuralgia
➤ proximal asymmetric diabetic
neuropathy
➤ entrapment neuropathy of an
anterior ramus of a
spinal nerve (T7−T12)
➤ pudendal neuralgia
➤ coccygodynia
➤
radicular syndrome
➤ herpes zoster
Clinical and Differential Diagnostic
Considerations
Neurogenic abdominal pain can
best be distinguished by the
type of pain.
➤ The stereotypical shooting pain of tabes
dorsalis, mostly in the mammary region, is rare.
➤ As indicated by its name, intercostal
neuralgia primarily manifests itself with
shooting pain, always at the same site. Coughing
and sneezing or pressure on the lateral
cutaneous ramus sometimes causes pain at its
passage. The cause of the pain may be a benign
chronic compressive radiculopathy from spinal
vertebra that have fused due to degenerative
processes, from thoracic disk hernia, rib
fracture or thoracotomy. Malignant compressive
radiculopathy from metastases, meningeal
carcinoma, Schwannoma, or a tuberculous lesion
should be considered.
➤ Only in the rare
"shingles without shingles" will the acute
herpes zoster pain pose diagnostic problems. The
abdominal pain precedes blister formation by
days. Borreliosis also causes intensive and
acute pain in the midsection but without skin
changes and can be diagnosed by serology.
➤
Asymmetric diabetic proximal neuropathy
(radiculopathy) is frequently not diagnosed.
Like borreliosis radiculitis, it frequently
begins unilaterally and later appears
contralaterally, and tends to occur segmentally,
to be localized in the abdominal region and
often lasts for months. Many abdominal signs and
symptoms are mistakenly attributed to
borreliosis because of the frequent severe pain
upon touching the skin, with allodynia or
hyperpathia. Importantly, diabetes may be only
mild. Asymmetric diabetic neuropathy is often
associated with a distal symmetric
polyneuropathy.
➤ A neuropathy of the
anterior rami of spinal nerves T7−T12 by
compression of the rectus abdominis muscle or by
overextension (e.g., during pregnancy) may cause
pain near the abdominal midline. A predisposing
polyneuropathy must be considered with such
unusual pressure or compression neuropathies.
➤ Perineal and genital lancinating or burning
pain with itching, numbness, or painful
sensitivity to touch indicate pudendal neuralgia
due to a lesion of one or both pudendal nerves,
rarely also with an initial caudal or plexus
process. Sitting becomes painful and sexual
activity impossible. Etiologic factors are
obstetric procedures, gynecologic, urologic or
proctologic conditions, surgery, perforating
trauma, and excessive horse or bicycle riding.
Unlike pudendal neuralgia, genitofemoral
neuralgia (ventrally) and coccygodynia
(dorsally) do not affect the perineal region.
➤ Coccygodynia, burning pain at the coccyx
caused in part by (secondary) arachnoidal growth
of sacral nerve roots, has primarily mechanical
causes such as a direct fall on the coccyx,
microtraumatization (television bottom), or
surgical procedures.
Nerve blockade or local
anesthesia often allow differentiation of this
pain.
➤ Pain in the abdominal region is also
frequently part of a radicular pain syndrome in
various spinal disorders,
particularly
spondylarthritis, discopathy, Bechterew disease,
osteoporosis, etc.
Please see also our Toxilact data base which is in the following language versions:
Toxilact Deutsche Sprachversion
Toxilact Nederlandstalige versie
Toxilakt έκδοση στην ελληνική γλώσσα
Toxilact English language version
Toxilact magyar nyelvű változat
Toxilact versione in lingua italiana
Toxilact polska wersja językowa
Detailed medical information on more common causes of acute abdomen
Intestinal Pain
Acute Appendicitis
Peritoneal Pain
Pain from Vascular Causes
Retroperitoneal Pain
Abdominal Pain from Intoxication
Toxicological risk during lactation
Toxicological lactation category I - the drug and/or its metabolites are either not eliminated through breast milk or are not toxic to the newborn and cannot lead to the development of absolutely any toxic reactions and adverse consequences for his health in the near and long term. Breast-feeding does not need to be discontinued while taking a given drug that falls into this toxicological lactation category.
Toxicological lactation category II - the drug and its metabolites are also eliminated through breast milk, but the plasma:milk ratio is very low and/or the excreted amounts cannot generate toxic reactions in the newborn due to various reasons, including degradation of the drug in the acid pool of the stomach of the newborn. Breastfeeding does not need to be discontinued while taking this medicine.
Toxicological lactation category III - the drug and/or its metabolites generate in breast milk equal to plasma concentrations or higher, and therefore the possible development of toxic reactions in the newborn can be expected. Breastfeeding should be discontinued for the period corresponding to the complete elimination of the drug or its metabolites from the mother's plasma.
Toxicological lactation category IV - the drug and/or its metabolites generate a plasma:milk ratio of 1:1 or higher and/or have a highly toxic profile for both the mother and the newborn, therefore their administration is incompatible with breastfeeding and it should to stop completely, and not just for the period of taking the drug, or to look for a less toxic therapeutic alternative.