Content
The content of medical knowledge in this section of the site of the Lactology Foundation is intended for the practical needs of doctors, pharmacists and students in these specialties. It is more than reasonable to consult other authoritative medical sources before using our medical knowledge.
- Lung in Health and Disease
- General Approach to Patients
With Respiratory Disorders - Evaluating Lung Structure and Function
- Interstitial Lung Diseases
- Pulmonary Vascular Diseases
- Disorders of the Pleura,
Mediastinum, and Chest Wall - Respiratory Failure
- Lung Transplantation
- Perioperative Pulmonary Management
- COVID-19 Pulmonary Management
- Congenital Lung Malformations
- Sleep-Related Disorders
Pulmonary Function Testing
They are used to establish baseline lung function, evaluate dyspnea, detect pulmonary disease, monitor effects of therapies used to treat respiratory disease, evaluate respiratory impairment or disability, evaluate operative risk, and perform surveillance for occupational-related lung disease. It may also be used in research and clinical trials and epidemiological surveys.
Spirometry
Description
Spirometry
assesses the integrated mechanical function of
the lung, chest wall, respiratory muscles, and
airways by measuring the total volume of air
exhaled from a full lung (total lung capacity
[TLC]) to maximal expiration (residual volume
[RV]). This volume, the forced vital capacity
(FVC) and the forced expiratory volume in the
first second of the forceful exhalation (FEV1),
should be repeatable to within 0.15 L upon
repeat efforts in the same measurement unless
the largest value for either parameter is less
than 1 L. In this case, the expected
repeatability is to within 0.1 L of the largest
value. The patient is instructed to inhale as
much as possible and then exhale rapidly and
forcefully for as long as flow can be
maintained. The patient should exhale until one
of the criteria defining the end of a forced
exhalation has been reached. At the end of the
forced exhalation, the patient should again
inhale fully as rapidly as possible. The FVC
should then be compared with that inhaled volume
to verify that the forced expiratory maneuver
did start from full inflation.
Reduction in
FEV1 may reflect reduction in the maximum
inflation of the lungs (TLC); obstruction of the
airways; respiratory muscle weakness; or
submaximal expiratory force due to poor
coaching, poor understanding, or malingering.
Airway obstruction is the most common cause of
reduction in FEV1. Airway obstruction may be
secondary to bronchospasm, airway inflammation,
loss of lung elastic recoil, increased
secretions in the airway, or any combination of
these causes. Response of FEV1 to inhaled
bronchodilators is used to assess the
reversibility of airway obstruction, although it
is now widely appreciated that a response
showing a lack of a significant increase in FEV1
does not indicate the patient will not benefit
clinically from bronchodilator therapy. A
significant increase in the inspiratory capacity
(IC) and/or vital capacity (VC) after
bronchodilator therapy can occur even when the
FEV1 fails to show a significant change.[1]
The standards used to describe the quality of
spirometry measurements are from the
Standardization of Spirometry 2019 Update.[2]
This document provides examples of the most
common technical problems associated with
spirometry testing. See Standardization of
Spirometry 2019 Update. An Official American
Thoracic Society and European Respiratory
Society Technical Statement for more
information.
Indications
Spirometry is
used to establish baseline lung function,
evaluate dyspnea, detect pulmonary disease,
monitor effects of therapies used to treat
respiratory disease, evaluate respiratory
impairment or disability, evaluate operative
risk, and perform surveillance for
occupational-related lung disease. It may also
be used in research and clinical trials and
epidemiological surveys.
Contraindications
Relative contraindications (no absolute
contraindications) for spirometry are as
follows:
• Conditions that may be negatively
impacted by the increases in myocardial demand
or changes in blood pressure associated with
spirometry: These include recent (< 1 week)
myocardial infarction, systemic hypotension or
severe hypertension, significant
atrial/ventricular arrhythmia, noncompensated
heart failure, uncontrolled pulmonary
hypertension, acute cor pulmonale, clinically
unstable pulmonary embolism, and a history of
syncope associated with forced exhalation.
•
Conditions that may be negatively impacted by
the increase in intracranial/intraocular
pressure associated with spirometry: These
include cerebral aneurysm, recent (< 4 weeks)
brain surgery, recent concussion with continuing
symptoms, and recent (within 1 week) eye
surgery.
• Conditions that may be negatively
impacted by increased sinus and middle ear
pressures: Examples include recent (< 1 week)
sinus or middle ear surgery or infections.
Conditions that may be negatively impacted by
increased intrathoracic and intraabdominal
pressures: Examples include the presence of
pneumothorax, recent (< 4 weeks) thoracic or
abdominal surgery, and late-term pregnancy.
• Infection control issues, including active or
suspected transmissible respiratory or systemic
infections
tuberculosis, or physical
conditions predisposing to transmission of
infections such as hemoptysis, significant
secretions or oral lesions or bleeding.
Patient care/preparations
Two choices are
available with respect to bronchodilator and
medication use prior to testing. Patients may
withhold oral and inhaled bronchodilators to
establish baseline lung function and evaluate
maximum bronchodilator response, or they may
continue taking medication as prescribed. If
medications are withheld, a risk of exacerbation
of bronchial spasm exists.
Interpretation
Interpretation of spirometry results should
begin with an assessment of test quality.
Failure to meet performance standards can result
in unreliable test results (see the image
below). The American Thoracic Society (ATS)
defines acceptable spirometry as an expiratory
effort that has the following characteristics:
Pulmonary function tests require patients to
successfully perform respiratory maneuvers in a
standardized manner in order to obtain
clinically meaningful results. Spirometry is
perhaps the most technically and physically
demanding. The patient is required to inhale as
fully as possible, exhale with as much force as
possible, and continue their expiratory effort
until they empty their lungs as completely as
possible or are unable to continue.
The
performance standards for acceptable spirometry
are summarized below. The comments of the
technologist administering the test can assist
the interpreting physician in determining if
results of a testing session that fail to meet
some of the standards can still provide
clinically useful data
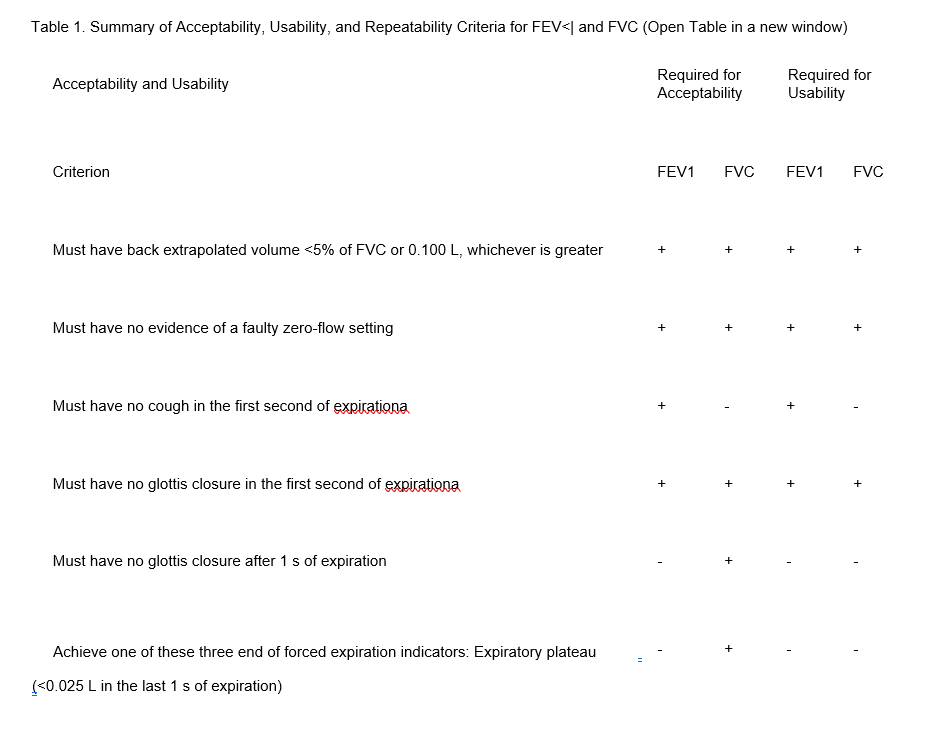
Age > 6 y: Difference between two largest FVC
values must be <0.150 L, and the difference
between two largest FEV1 values must be <0.150 L
Age <6 y: Difference between two largest FVC
values must be <0.100 L or 10% of the highest
value, whichever is greater, and the difference
between two largest FEV1 values must be <0.100 L
or 10% of the highest value, whichever is
greater aFor children <6 y, must have at least
0.75 s of expiration without glottis closure or
cough for acceptable or usable measurement of
FEV0.75.
bOccurs when the patient cannot
expire long enough to achieve a plateau (eg,
children with high elastic recoil or patients
with restrictive lung disease) or the patient
inspires or comes off the mouthpiece before a
plateau. For within-maneuver acceptability, the
FVC must be larger than or within the
repeatability tolerance of the largest FVC
observed before this maneuver within the current
prebronchodilator or the current
postbronchodilator testing set.
cAlthough the
performance of a maximal forced inspiration is
strongly recommended, its absence does not
preclude a maneuver from being judged
acceptable, unless extrathoracic obstruction is
specifically being investigated.
Characteristics of acceptable spirometry
efforts are as follows:
• The patient is
vigorously coached to inspire rapidly to full
inflation.
• The patient shows minimal
hesitation at the start of the forced expiration
(extrapolated volume < 5% of FVC or 0.10 L,
whichever is larger).
• The patients show an
explosive start of the forced exhalation (rise
time to peak flow no greater than 0.150 s). Rise
time to peak flow is not available on all
spirometers. If it is not available, it is not
part of the assessment of the acceptability of
the start of the forced exhalation.
• The
patient shows no evidence of cough or artifact
in the first second of forced exhalation.
•
The results meet one of three criteria that
define a valid end-of-forced exhalation: (1)
smooth curvilinear rise of the volume-time
tracing to a plateau (plateau defined as < 0.025
L volume change in the last 1 s of expiration )
of at least 1 second's duration; (2) if a forced
test fails to exhibit an expiratory plateau, a
forced expiratory time of 15 seconds; or (3) the
FVC is within the repeatability tolerance of or
is greater than the largest prior observed FVC.
• Upon completing the forced exhalation, the
patient is coached to rapidly (> 2 L/s flow)
inhale to full inflation upon completing the
forced exhalation providing a value for forced
inspiratory vital capacity (FIVC). The maximum
FIVC can be no more than 0.100 L or 5% of the
FVC larger than the FVC (whichever is greater).
If the maximum FIVC is more than 0.100 L or 5%
of the FVC greater than the FVC, that effort is
not acceptable and cannot be used for reporting
of any parameters.
• Repeatability of the
largest FVC and FEV <| within 0.150 L (within
0.100 L if age < 6 y) is demonstrated in at
least two efforts.
In patients who have significant loss of lung
elastic recoil (pulmonary emphysema, COPD),
spirometry may show negative effort dependence
of forced expiratory flow. The effort that has
the highest peak expiratory effort may produce a
lower FEV1 because of the dynamic compression of
the airways that results from the loss of
elastic recoil support of airways that is
characteristic of emphysema. In this
circumstance, reporting the highest FEV1 coming
from an effort with submaximal expiratory effort
can lead to confusing results, particularly if a
setting of assessing spirometric response to
bronchodilators. Although not yet a spirometry
acceptability standard, it appears that when
reporting the FEV1 considering only efforts that
have a time to peak flow (TPEF) less than or
equal to 0.12 seconds helps eliminate this
effect. This parameter can be displayed on most
laboratory-based spirometry testing systems.
Inspection of the volume-time tracing aids in
identification of early termination of
expiration by evaluating the presence of an
expiratory plateau. In the absence of an
expiratory plateau, a 15-second expiratory time
ensures the quality of the FVC. Inspection of
the start of the volume-time tracing can help
identify a hesitant start, which can result in a
falsely low FEV1. Repeatability of the FVC and
the FEV1 helps ensure that the results truly
represent the patient's lung function. Attention
should be focused on the repeatability of two
key parameters: FVC and FEV1. It should be noted
that while repeatability of the FVC and FEV1
strengthens the confidence that the forced
exhalations started from full inflation, it is
possible to demonstrate repeatability of these
parameters even when forced exhalations start
from a lung volume below full inflation.
Demonstration that the difference between the
largest FIVC and the FVC is no more than the
larger of 0.100 L or 5% of the largest FIVC is a
key acceptability criterion.
The reference
equations published in 2012 by the Global Lung
Initiative (GLI), a Task Force of the European
Respiratory Society, provide normative values
for males and females from age 3 to 95 years
across a wide range of ethnicities,[3] and these
should be used as the default set of reference
values for spirometry. The use of these
predicted values for spirometry has been
supported globally, including endorsements from
the European Respiratory Society, the ATS, the
American College of Chest Physicians, the
Thoracic Society of Australia and New Zealand,
the Australian and New Zealand Society of
Respiratory Science, and the Asian Pacific
Society for Respirology. The report is in
accordance with the previously published
recommendations of the ATS that called for the
elimination of a fixed percentage of predicted
cut point to determine normality and a fixed
lower limit of normal of the FEV1/FVC ratio to
identify airway obstruction, both of which have
been shown to result in significant
misclassification of spirometry results.
Guidelines for a standardized report format have
been published and should be the default report
format. The use of Z scores to determine the
severity of spirometric abnormalities is
encouraged.
Abnormalities can be classified
by the physiological patterns outlined below.
Obstructive defects
Disproportionate
reduction in the FEV1 as compared with the FVC
is reflected in the FEV1/FVC ratio and is the
hallmark of obstructive lung diseases. This
physiologic category of lung diseases includes
but is not limited to asthma, acute and chronic
bronchitis, emphysema, bronchiectasis, cystic
fibrosis, and bronchiolitis. The forced
expiratory flow at any given lung volume is
reduced. The mechanism responsible for the
reduction in airflow can be bronchial spasm,
airway inflammation, increased intraluminal
secretions, and/or reduction in parenchymal
support of the airways due to loss of lung
elastic recoil. Poor understanding and effort on
the part of the patient is also a cause for
reduced flows, and the diagnosis of airway
obstruction should be limited to measurements
composed of acceptable efforts demonstrating
repeatability of FVC and FEV1.
The use of a
fixed lower limit of normal for the FEV1/FVC
ratio as proposed by the Global Initiative for
Obstructive Lung Disease (GOLD) lacks a
scientific basis and results in significant
misclassification of patients at either end of
the age spectrum. Young patients are classified
as "normal" when airflow obstruction is present,
and older patients are classified as showing
obstruction when no airflow obstruction is
present. The use of the GOLD threshold for
identifying airway obstruction should be
discouraged in clinical practice where or when
computerized predicted values are available.
The recommended practice for identifying a
spirometric abnormality is to use the predicted
lower limit of normal for that individual based
on sex, age, height, and ethnicity. The GLI
reference equations provide lower limits of
normal for spirometric parameters.
Sient of reversibility of airway obstruction
ay obstruction is identified on spirometry,
assessing response to inhaled bronchodilators is
useful. The ATS has ded that the threshold for
significant response be demonstration of an
increase of at least 12% and 0.2 L in either FVC
(provided the expiratory time for both sessions
agree within 10%) or FEV1 on a spirogram
performed 10-15 minutes after inhalation of a
therapeutic dose of a bronchodilating agent. New
standards recommend the use of four inhalations
(100 meg each, 400 meg total dose) of albuterol
administered through a valved spacer device.
When concern about tremor or heart rate exists,
lower doses may be used. Response to an
anticholinergic drug may be assessed 30 minutes
after four inhalations (40 meg each, 160 meg
total dose) of ipratropium bromide. Failure to
respond to bronchodilator challenge does not
preclude clinical benefit from bronchodilators.
A positive response to the bronchodilators may
correlate with response to steroid therapy.
Restrictive defects
Reduction in the FVC
with a normal or elevated FEV1-to-FVC ratio
should trigger further evaluation of total lung
capacity (TLC) to rule out restrictive lung
disease. Measuring the TLC and residual volume
(RV) can confirm restriction suggested by
spirometry
Normal aging results in an
increase in functional reserve capacity (FRC)
and residual volume (RV) and a normal total lung
capacity (TLC) percentage. Obstructive lung
diseases cause hyperinflation (increase in RV
and FRC) with a relatively normal forced vital
capacity (FVC). In severe emphysema, the TLC
percentage can exceed 150%, with the RV
impinging on the FVC. Restrictive lung diseases
exhibit reduced TLC percentage with relative
preservation of the RV/TLC percentage in
fibrosis, a reduced inspiratory capacity and
expiratory reserve volume (ERV) in neuromuscular
disease, and severe reduction of the ERV in
extreme obesity.
Quantification of impairment by spirometry
In normal spirometry, FVC, FEV1, and FEV1
-to-FVC ratio are above the lower limit of
normal. The lower limit of normal is defined as
the result of the mean predicted value (based on
the patient's sex, age, and height) minus 1.64
times the standard error of the estimate from
the population study on which the reference
equation is based. If the lower limit of normal
is not available, the FVC and FEV1 should be
greater than or equal to 80% of predicted, and
the FEV1 -to-FVC ratio should be no more than
8-9 absolute percentage points below the
predicted ratio. The ATS has recommended the use
of lower limits of normal instead of the 80% of
predicted for setting the threshold that defines
abnormal test results.
A reduced FVC on
spirometry in the absence of a reduced FEV1/FVC
ratio suggests a restrictive ventilatory
problem. An inappropriately shortened exhalation
during spirometry can (and often does) result in
an artifactually reduced FVC. Causes of
restriction on spirometry include obesity,
cardiomegaly, ascites, pregnancy, pleural
effusion, pleural tumors, kyphoscoliosis,
pulmonary fibrosis, neuromuscular disease,
diaphragm weakness or paralysis, space-occupying
lesions, lung resection, congestive heart
failure, inadequate inspiration or expiration
secondary to pain, and severe obstructive lung
disease. One scheme for describing the severity
of reductions in the FVC and/or the FEV1 is
shown below:
• Mild - Greater than 70% of
predicted
• Moderate - 60-69% of predicted
• Moderately severe - 50-59%
• Severe -
35-49% of predicted
• Very severe - Less than
35% of predicted
The lower limit of normal for the FEF25-75% can be less than 50% of the mean predicted value, making it important to use the lower limit of normal defined by the 95% confidence limit of the mean predicted value rather than a threshold defined by a fixed percentage of the predicted value. The FEF25-75% is also very dependent on expiratory time. If expiratory times of spirometry efforts vary by more than 10%, comparisons of the FEF25-75% before and after bronchodilator challenge are difficult to Early termination of expiration shifts the middle 50% of the exhaled volume towards the start of the exhalation, ill raising the FEF25-75%. For these reasons, the use of the FEF25-75% to assess airway function in adults is indicated.
The lower limit of normal for the FEF25-75% can be less than 50% of the mean predicted value, making it important to use the lower limit of normal defined by the 95% confidence limit of the mean predicted value rather than a threshold defined by a fixed percentage of the predicted value. The FEF25-75% is also very dependent on expiratory time. If expiratory times of spirometry efforts vary by more than 10%, comparisons of the FEF25-75% before and after bronchodilator challenge are difficult to Early termination of expiration shifts the middle 50% of the exhaled volume towards the start of the exhalation, ill raising the FEF25-75%. For these reasons, the use of the FEF25-75% to assess airway function in adults is indicated. The FVC is a reliable means of assessing the clinical status in idiopathic pulmonary fibrosis (IPF). A minimum clinically important difference of the FVC, expressed as a percentage of the mean predicted normal value, of 2-6% has been established. This obviates the need to obtain a total lung capacity (TLC) measurement to assess disease progression or the effects of medical therapy.
Special assessments
Sitting versus supine
vital capacity
Evaluation of diaphragm
strength can be accomplished by measuring the
vital capacity in an upright or sitting position
followed by a measurement made in the supine
position. A reduction in the vital capacity to
less than 90% of the upright vital capacity
suggests diaphragm weakness or paralysis.
Interpreting an increased reduction in vital
capacity in the supine position as diaphragm
dysfunction should be made cautiously if the
patient's body mass index is greater than 45
kg/m2.[4] Studies reporting the normal reduction
of the vital capacity of less than 10% from
upright to supine were conducted with
individuals who were not obese. Slightly greater
reductions in obese individuals in a supine
position may not indicate diaphragm dysfunction,
but rather an increase in the resistive forces
against which the diaphragm descends. Reductions
in the supine vital capacity more than 20% of
baseline indicate hemidiaphragm or diaphragm
dysfunction or paralysis.
Identifying central
airway obstructions
The configuration of the
flow-volume curve of a properly performed
spirometry test can be used to demonstrate
various abnormalities of the larger central
airways (larynx, trachea, right and left
mainstem bronchi). Three patterns of flow-volume
abnormalities can be detected: (1) variable
intrathoracic obstructions, (2) variable
extrathoracic obstructions, and (3) fixed upper
airway obstructions. Reproducing these findings
on every effort is important because spurious
nonreproducible reductions in inspiratory flow
are not uncommon after completion of forced
expirations in subjects without upper airway
obstruction. Examples of variable intrathoracic
obstruction include localized tumors of the
lower trachea or mainstem bronchus,
tracheomalacia, and airway changes associated
with polychondritis.
Variable upper airway
obstructions demonstrate flow reductions that
vary with the phase of forced respirations.
Variable intrathoracic obstructions demonstrate
reduction of airflow during forced expirations
with preservation of a normal inspiratory flow
configuration. This is observed as a plateau
across a broad volume range on the expired flow
limb of the flow-volume curve. The reduction in
airflow results from a narrowing of the airway
inside the thorax, in part because of a
narrowing or collapse of the airway secondary to
extraluminal pressures exceeding intraluminal
pressures during expiration.
Variable
extrathoracic obstructions demonstrate reduction
of inspired flows during forced inspirations
with preservation of expiratory flows. Again,
the major cause of the reduced flow during
inspiration is airway narrowing secondary to
extraluminal pressures exceeding intraluminal
pressures during inspiration. Causes of this
type of upper airway obstruction include
unilateral and bilateral vocal cord paralysis,
vocal cord adhesions, vocal cord constriction,
laryngeal edema, and upper airway narrowing
associated with obstructive sleep apnea. Fixed
upper airway obstructions demonstrate plateaus
of flow during both forced inspiration and
forced expiration. Causes of fixed upper airway
obstruction include goiters, endotracheal
neoplasms, stenosis of both main bronchi,
postintubation stenosis, and performance of the
test through a tracheostomy tube or other fixed
orifice device. Flow reduction must be
consistent on every effort to be considered
actual flow limitation. Fixed upper airway
obstruction may be caused by postintubation
stenosis, goiter, endotracheal neoplasms, and
bronchial stenosis. Variable intrathoracic
obstruction may be caused by tracheomalacia,
polychondritis, and tumors of the lower trachea
or main bronchus. Variable extrathoracic
obstruction may be caused by bilateral and
unilateral vocal cord paralysis, vocal cord
constriction, reduced pharyngeal cross-sectional
area, and airway burns. While no single test can
effectively predict intraoperative and
postoperative morbidity and mortality from
pulmonary complications, the FEV1 obtained from
good quality spirometry is a useful tool. When
the FEV1 is greater than 2 L or 50% of
predicted, major complications are rare.
Operative risk is heavily dependent on the
surgical site, with chest surgery having the
highest risk for postoperative complications,
followed by upper and lower abdominal sites.
Patient-related factors associated with
increased operative risk for pulmonary
complications include preexisting pulmonary
disease, cardiovascular disease, pulmonary
hypertension, dyspnea upon exertion, heavy
smoking history, respiratory infection, cough
(particularly productive cough), advanced age
(>70 y), malnutrition , general debilitation,
obesity, and prolonged surgery.
Assessment
for lung surgery typically involves prediction
of a postoperative FEV1 by using the
preoperative FEV1. In a borderline case,
consideration of the contribution of the
remaining portions can be assessed by a
perfusion scan. The relative percentage of
perfusion (Q) of the remaining lung or lung
segments usually is proportional to its
contribution to ventilation and can be used to
estimate postoperative function as shown in the
following equation:
Postoperative FEV1 =
Preoperative FEV1 x Q% of the remaining lung
For example, if the preoperative FEV1 is 1.6 L
and the lung to be resected demonstrates 40%
perfusion, the postoperative FEV1 would be 1.6 x
0.6 = 0.96 L. An estimated postoperative FEV1 of
less than 0.8 L is often associated with chronic
respiratory failure and may indicate an
unacceptable degree of operational risk.
Arterial blood gases (ABGs) and cardiopulmonary
exercise testing may help evaluate operative
risk in patients who have a preoperative FEV1
below 2 L or 50% of predicted.
The algorithm
for clearance of candidates for lung resection
proposed by Bolinger and Perruchoud[5] has been
successfully evaluated in 137 consecutive
patients who were referred for resection by
Wyser et al[6] with an overall mortality of 1.5%
and is detailed in Cardiopulmonary Stress
Testing. Patients with a negative cardiac
history and ECG that demonstrate an FEV1 and a
diffusing capacity of lung for carbon monoxide
(DLCO) that are greater than 80% of predicted
are judged to be able to undergo pneumonectomy
safely.
Lung Volume Determination
Synonyms
Functional reserve capacity (FRC), helium
dilution lung volumes, nitrogen washout lung
volumes, static lung volumes, lung subdivisions
Indications
Lung volume determinations are
used in the evaluation of suspected restrictive
lung disease and the evaluation of
hyperinflation.
Contraindications
Inability to follow instructions is a
contraindication. Patients with claustrophobia
may not tolerate being closed into a confined
space (body plethysmograph), but anxiety can
often be overcome with good instruction and
coaching.
Diffusing Capacity of Lung for Carbon
Monoxide
Synonyms
Transfer factor of the
lung for carbon monoxide (TLCO,
mmol/min/kilopascal, commonly used in Europe);
DLCO, diffusing capacity of lung for carbon
monoxide (DL, mL/min/mmHg); transfer coefficient
of the lung for carbon monoxide (KCO); and
alveolar volume (VA, L), which is the
single-breath estimate of the TLC determined by
the dilution of the tracer gas concentration.
The term KCO should be used instead of the term
DLCOA/A, which incorrectly implies that the DLCO
is being corrected for lung volume.
Contraindications
Inability to follow
instructions is a contraindication to a DLCO
test (CPT code 94729). Patients should be alert,
oriented, able to exhale completely and inhale
to total lung capacity, able to maintain an
airtight seal on a mouthpiece, and able to hold
a large breath for 10 seconds.
Patient
care/preparations
Refrain from smoking for
several hours before the test. Alcohol vapors
can affect the accuracy of some fuel cell types
of CO analyzers, thus alcoholic beverages should
be withheld for eight hours.
Test
DLCO,
also known as the TLCO, is a measurement of the
conductance or ease of transfer for CO molecules
from alveolar gas to the hemoglobin of the red
blood cells in the pulmonary circulation. It is
often helpful for evaluating the presence of
possible parenchymal lung disease when
spirometry and/or lung volume determinations
suggest a reduced vital capacity, RV, and/or
TLC. It should be noted that different units of
measure exist worldwide. In the United States,
the test is known as the DLCO and the units of
measure are mL/min/mm Hg (traditional unit of
measure). In contrast, the test is also known as
the TLCO and the units of measure are
mmol/min/kPa (International System of Units or
SI units). The conversion from SI units
(mmol/min/kPa) to traditional (mL/min/mm Hg) can
be done by multiplying the SI value by 2.987.
Recommendations for a standard technique for the
test were first published by the American
Thoracic Society (ATS) in 1995. A joint task
force from the ATS and the European Respiratory
Society (ERS) published updated standards in
2017.[7] The updated standards include some
important changes in the criteria used to
determine the technical acceptability and
expected repeatability of measurements, as well
as recommendations on the increased utility of
the procedure when rapid-responding gas analyzer
(RGA) technology is used. RGA technology has
been available for over a decade and most
commercial equipment currently sold uses the RGA
technology. It is likely that most of the
slower-responding analyzer technology will be
phased out by equipment replacement over the
coming decade.
Most pulmonary laboratories
perform this test by the single-breath technique
(DLCO SB) because it is quicker to perform and
more reproducible than other techniques. Other
techniques, such as the rebreathing technique,
are not commonly available and are not described
here. In the single-breath technique, the
subject exhales to RV and then inhales the test
gas (tracer gas, [commonly either 10% helium or
0.3% methane], 0.3% CO, 21% oxygen, and balance
nitrogen) briskly to TLC. This vital
capacity-size breath is held for 10 seconds and
then exhaled either into a sample bag (discrete
sampling) or past a sampling port leading to
rapid-response analyzers after an initial
discard of 0.75-1 L of the exhale to minimize
the contribution of dead space gas (mouthpiece,
filter, measuring equipment, and anatomical
areas where no gas exchange is expected) to the
gas sample that will be analyzed to estimate
uptake of CO by the alveolar capillaries. The
grab sample (0.75-1 L) is then analyzed gas and
CO. The dilution of the tracer gas in the vital
capacity-size breath of test gas by the
patient's RV provides means to estimate the
initial alveolar concentration of CO and to
estimate the patient's lung volume at full
inflation. The ffusion of the CO can be
estimated by the change from this initial
alveolar concentration to that of the expired
grab. This change in the CO concentration is
then multiplied by the single-breath estimate of
TLC to calculate the diffusing capacity.
Abnormal hemoglobin (Hb) levels can affect the
diffusing capacity and, if known, should be used
to mathematically correct the measured diffusing
capacity to what it would be if the patient's
hemoglobin was normal. Although it has been
recommended that the predicted value be adjusted
for hemoglobin,[7, 8] providing an estimate of
what the patient's expected DLCO should be given
their hemoglobin level, equipment manufacturers
have been slow to offer this accommodation in
the testing software and the older practice of
adjusting the patient's measured DLCO to what it
would be if their hemoglobin was normal is still
quite common. Both methods are presented below.
Both methods yield identical values when the
measured values are compared with the predicted
values and expressed as a percentage of the
predicted value. Regardless of whether the
measured or predicted values are adjusted, both
adjusted and unadjusted values should be
displayed on the final report, along with the
measured hemoglobin (and date of hemoglobin
determination).
Adjusting the patient's
measured DLCO value for the measured hemoglobin
(not currently recommended but still commonly
used) is as follows:
• Adolescent males and
men: Hb adjusted DLCO (DLCOc) = measured DLCO
([10.22 + Hb g/dL]/[1.7 Hb])
• Children
younger than 15 years and women: Hb adjusted
DLCO (DLCOc) = measured DLCO ([9.38 + Hb
g/dL]/[1.7 Hb])
Adjusting the predicted DLCO
(and lower limit of normal) for the patient's
measured hemoglobin (currently recommended) is
as follows:
• Adolescent males and men: DLCO
(predicted for Hb) = DLCO (predicted) x (1.7
Hb/(10.22 + Hb))
• Children younger than 15
years and women: DLCO (predicted for Hb) = DLCO
(predicted) x (1.7 Hb/(9.38 + Hb))
Other
factors have been shown to impact the measured
DLCO, such as elevated blood carboxyhemoglobin
(COHb) and barometric pressure. The impact of an
elevated carboxyhemoglobin is twofold: (1) it
reduces the alveolar-capillary pressure gradient
for CO and (2) acts as a virtual anemia by
holding onto sites on the hemoglobin molecule
that could be used for binding CO (or oxygen) .
The net effect is a 2% decrease in DLCO for each
1% increase in COHb. RGA systems can measure the
CO in the patient's exhaled breath just prior to
inhalation of the DLCO test gas and compensate
for elevated CO by subtracting the estimated CO
back-pressure from both the initial and final
alveolar carbon monoxide partial pressures. This
compensates for the reduced alveolar-capillary
pressure gradient but does not compensate for
the anemia effect. The 2017 DLCO standards paper
shows a formula that also adjusts for the anemia
effect, but this is not currently in use on most
PFT systems.
The current recommendation is to
correct the measured DLCO for barometric
pressure. As barometric pressure falls, so does
the partial pressure of inspired oxygen (PI02)
and DLCO increases. The typical variation in
DLCO expected from atmospheric pressure
fluctuation at a given altitude is +1.5%.
Laboratories at higher altitude can produce
higher values; the expected change is
approximately 0.5% for each 100-meter increase
in altitude. This adjustment can only be made if
the barometric pressure is made or updated in
the measuring system on a daily basis.
Quality grading for DLCO maneuvers
The
2017 ATS/ERS DLCO standards paper specified
changes to the acceptability and repeatability
standards used to determine technical
acceptability.^] It also proposed a quality
control grading system that acknowledges that
test results from efforts that fail to meet all
of the acceptability criteria may still provide
clinically useful data.
The 2017 criteria for
acceptability of DLCO efforts are as follows:
• VI (inspired volume of test gas) greater than
90% of the largest VC measured by same-day slow
or forced spirometry (2005 standard was >85%) or
• VI greater than 85% of largest VC and alveolar
volume (VA) within 0.2 L or 5% (whichever is
greater) of the largest VA from other acceptable
maneuvers
• 85% of test gas VI inhaled in
less than 4 seconds (unchanged from 2005
standards)
• Breathe hold time of 10 + 2
seconds without evidence of significant leaks,
Valsalva maneuver, or Mueller maneuver
(unchanged from 2005 standards)
• Sample
collection completed within 4 seconds of the
start of exhalation (was 3 seconds in 2005
standards); for RGA systems, virtual sample
collection should be initiated after dead-space
washout is complete
The 2017 criterion for
DLCO repeatability is as follows:
• At least
two acceptable DLCO measurements within 2
mL/min/mm Hg (0.67 mmol/min/kPa) of each other
(2005 standard was 3 mL/min/mm Hg or 1
mmol/min/kPa)
Quality grading for DLCO measurements is as
follows:
• Score of A: (1) VI/VC 90% or VI/VC
greater than 85% and VA within 0.2 L or 5% of
largest VA from another acceptable aneuver; (2)
breath hold time of 8-12 seconds; and (3) sample
collection less than 4 seconds blore of B: (1)
VI/VC greater than 85%; (2) breath hold time of
8-12 seconds; and (3) sample collection less
than 4 icons
• Score of C: (1) VIA/C greater
than 80%; (2) breath hold time of 8-12 seconds;
and (3) sample collection less than 5 seconds
• Score of D: (1) VIA/C greater than 80%; (2)
breath hold time of less than 8 seconds or
greater than 12 seconds; and (3) sample
collection less than 5 seconds
• Score of F:
(1) VI/VC less than 80%; (2) breath hold time of
less than 8 seconds or greater than 12 seconds;
and (3) sample collection greater than 5 seconds
Only grade A maneuvers meet all acceptability
criteria. The average DLCO values from two or
more grade A maneuvers that meet the
repeatability criterion should be reported. If
only one grade A maneuver is obtained, the DLCO
value from that maneuver should be reported. If
no grade A maneuver is obtained, maneuvers of
grades B to D might still have clinical utility,
and the average of such maneuvers should be
reported. However, these deviations from the
acceptability criteria must be noted to caution
the interpreter of the test. Maneuvers of grade
F are not usable.
Results
The 2017 ATS recommendations for a
standardized pulmonary function report details
recommendations for reporting of DLCO. A major
change is the recommendation to express the
measured DLCO on a z-score scale, which
expresses the result as the number of multiples
of a standard deviation above or below a
population mean.
When hemoglobin is measured
and available, it should be shown on the report
with a note indicating whether the measured or
predicted value has been adjusted for this.
Interpretation
Because the DLCO is
directly proportional to VA (VA is the lung
volume after inhalation of the DLCO test gas,
based on the size of the breath of test gas and
the dilution of the inspired tracer gas).
Nonpulmonary processes that reduce the lung
volume at full inflation cause reductions in the
DLCO. If VA can be assessed accurately, these
reductions produce a normal or elevated KCO.
Examples of this include lung resection,
thoracic cage abnormalities (eg,
kyphoscoliosis), and small lungs. DLCO is
reduced in pulmonary emphysema. However, because
of the poor distribution of the inspired test
gas, the VA may grossly underestimate the TLC,
and the resulting KCO may be normal. A reduced
DLCO and a reduced KCO suggest a true
interstitial disease such as pulmonary fibrosis
or pulmonary vascular disease. It has
demonstrated that in healthy patients, the KCO
is increased to above normal levels when the
DLCO test is performed at volumes less than the
TLC.
The pattern of a low DLCO and a normal
KCO may not be sufficient to rule out the
presence of parenchymal disease. The works of
Johnson[9] and Chinn et al[10] advocate the
volume correction of the predicted value for
DLCO by using the measured VAto "correct" the
predicted DLCO for low or high lung volumes.
Further work is warranted, but studies
demonstrating the nonlinearity of the
relationship between lung volume and DLCO are
sufficiently convincing that the practice of
interpreting a low DLCO and a normal KCO
(previously known as DLCO/VA) as "normal" is
discouraged. The degree of severity of reduction
in the diffusing capacity can be assigned
according to the following scheme: less than the
predicted lower limit of normal but greater than
60% of predicted is mild, between 40% and 60% of
predicted is moderate, and less than 40% is
severe.
Nonperfusion of ventilated alveoli,
such as in pulmonary vascular disease, produces
a reduction of both the DLCO and the KCO. Anemia
produces a virtual reduction in pulmonary
capillary blood volume that causes a reduction
in DLCO that can be adjusted mathematically for
the reduced hemoglobin. The DLCO may be reduced
temporarily in a variety of disorders such as
pneumonia, interstitial infiltrative disorders,
and alveolar proteinosis. The importance of
obtaining an inspiratory vital capacity (IVC)
greater than 90% of the best measured VC from
the day of the test cannot be overemphasized.
Inability to achieve an IVC of greater than or
equal to 90% of the largest VC measured that day
must be noted on the report.
Please see also our Toxilact data base which is in the following language versions:
Toxilact Deutsche Sprachversion
Toxilact Nederlandstalige versie
Toxilakt έκδοση στην ελληνική γλώσσα
Toxilact English language version
Toxilact magyar nyelvű változat
Toxilact versione in lingua italiana
Toxilact polska wersja językowa
Pulmonary symptoms, findings and investigations
Assessment of chronic cough
Expectoration
Hemoptysis
Pleural Effusion
Approach to wheezing in children
Polysomnography
Pulmonary Function Testing
Toxicological risk during lactation
Toxicological lactation category I - the drug and/or its metabolites are either not eliminated through breast milk or are not toxic to the newborn and cannot lead to the development of absolutely any toxic reactions and adverse consequences for his health in the near and long term. Breast-feeding does not need to be discontinued while taking a given drug that falls into this toxicological lactation category.
Toxicological lactation category II - the drug and its metabolites are also eliminated through breast milk, but the plasma:milk ratio is very low and/or the excreted amounts cannot generate toxic reactions in the newborn due to various reasons, including degradation of the drug in the acid pool of the stomach of the newborn. Breastfeeding does not need to be discontinued while taking this medicine.
Toxicological lactation category III - the drug and/or its metabolites generate in breast milk equal to plasma concentrations or higher, and therefore the possible development of toxic reactions in the newborn can be expected. Breastfeeding should be discontinued for the period corresponding to the complete elimination of the drug or its metabolites from the mother's plasma.
Toxicological lactation category IV - the drug and/or its metabolites generate a plasma:milk ratio of 1:1 or higher and/or have a highly toxic profile for both the mother and the newborn, therefore their administration is incompatible with breastfeeding and it should to stop completely, and not just for the period of taking the drug, or to look for a less toxic therapeutic alternative.